Pulsus Paradoxus: When Inspiration Makes the Pulse Disappear
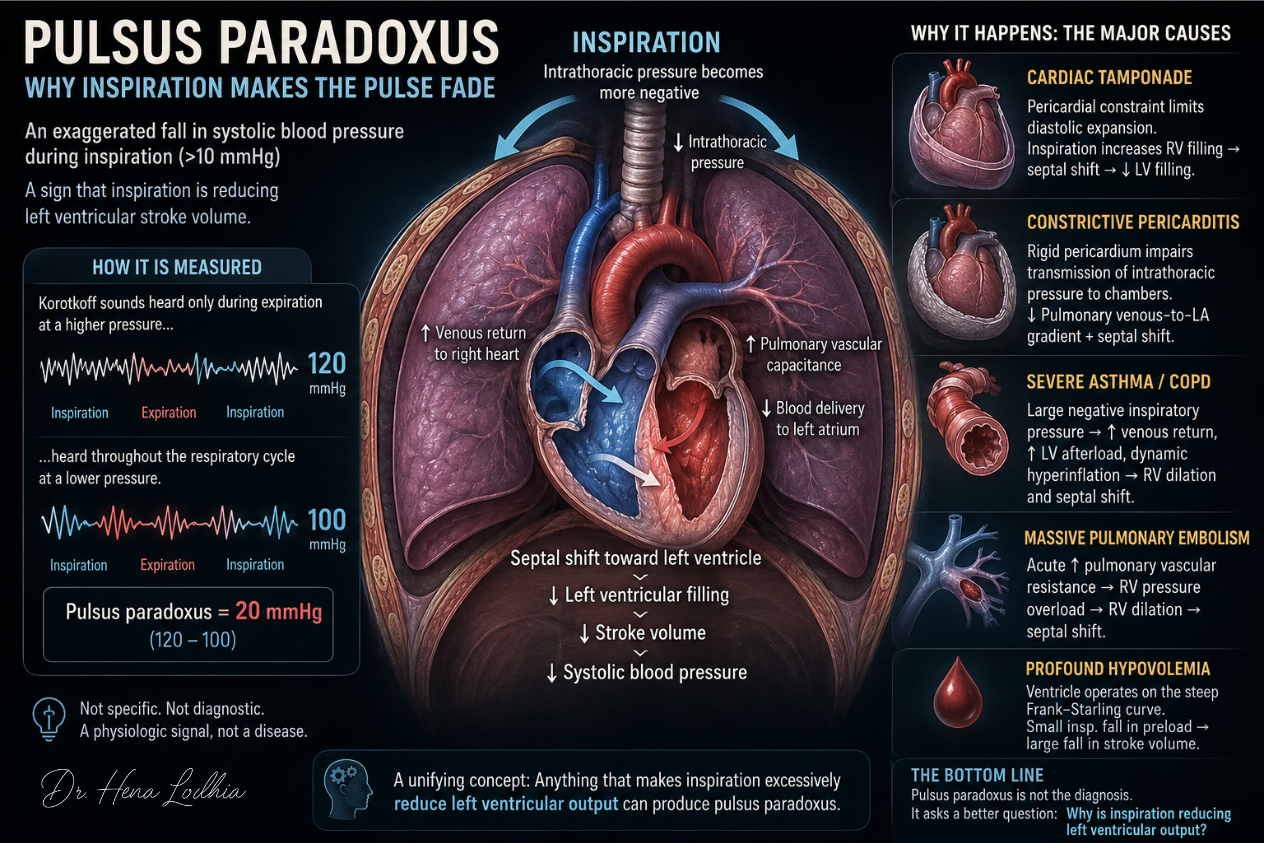
Pulsus paradoxus is often defined as an inspiratory fall in systolic blood pressure greater than 10 mmHg.
The definition describes what happens. It does not explain why it happens.
🎧 Clinical Summary Audio
Listen to the key concept in under 60 seconds.
The more useful question is this:
Why would inspiration make the left ventricle eject less blood?
That question matters more than the number itself. In modern practice, suspected cardiac tamponade is usually evaluated with point-of-care ultrasound or echocardiography, not by carefully measuring Korotkoff sounds with a sphygmomanometer. Ultrasound can rapidly show pericardial effusion, right atrial collapse, right ventricular diastolic collapse, a plethoric inferior vena cava, and Doppler respiratory variation in flow.
So why learn pulsus paradoxus at all?
Because the physiology behind it remains central to clinical medicine. Pulsus paradoxus is a visible expression of ventricular interdependence, pericardial constraint, respiratory variation in venous return, left ventricular transmural pressure, and the hemodynamic effects of severe obstructive lung disease.
The bedside maneuver has become less central.
The physiology has not.
The Historical Paradox
The term pulsus paradoxus was introduced by Adolf Kussmaul in the nineteenth century.
The paradox was not that the heart stopped during inspiration. The heart continued to beat. What seemed paradoxical was that the peripheral pulse weakened or disappeared during inspiration despite ongoing cardiac activity.
Modern physiology has clarified the observation.
The pulse fades because systolic pressure falls during inspiration. When this inspiratory fall exceeds the normal range, classically more than 10 mmHg, it is called pulsus paradoxus.
The name is historical. The mechanism is not paradoxical.
What Normally Happens During Inspiration
Spontaneous inspiration begins with diaphragmatic contraction.
Intrathoracic pressure becomes more negative. This increases the pressure gradient between the systemic veins and the right atrium, so venous return to the right heart increases.
At the same time, lung expansion transiently increases the capacitance of the pulmonary vascular bed. Some blood is temporarily held within the pulmonary circulation before returning to the left atrium. Left-sided filling therefore decreases slightly during early inspiration.
The two ventricles are not independent structures. They share the interventricular septum, sit within the same pericardial space, and influence each other during diastole. When right ventricular filling increases, the septum can shift slightly toward the left ventricle, reducing left ventricular filling.
In healthy individuals, these effects are small.
Inspiration slightly increases right ventricular filling, slightly reduces left ventricular preload, slightly lowers left ventricular stroke volume, and produces a small fall in systolic blood pressure.
Usually, this fall is less than 10 mmHg.
Pulsus paradoxus is not a new physiological process. It is an excessive version of this normal respiratory-cardiac interaction.
The Central Mechanism
All important causes of pulsus paradoxus converge on the same endpoint:
During inspiration, left ventricular stroke volume falls more than normal.
This can happen through three broad mechanisms.
First, inspiration may reduce left ventricular preload.
Second, inspiration may increase left ventricular afterload.
Third, inspiration may intensify ventricular interdependence, so that right ventricular filling occurs at the expense of left ventricular filling.
The magnitude of pulsus paradoxus is determined by how strongly the right and left ventricles compete for a limited diastolic volume and how severely respiration alters cardiac loading conditions.
That is the unifying idea.
Cardiac Tamponade: Competition Inside a Fixed Pericardial Space
Cardiac tamponade is the classic setting for pulsus paradoxus.
The key problem is not merely pericardial fluid. The key problem is pressure. Tamponade develops when pericardial pressure rises enough to restrict diastolic filling.
Once the pericardium reaches the steep part of its pressure-volume curve, small increases in pericardial volume cause large increases in intrapericardial pressure. The cardiac chambers can no longer expand normally during diastole.
The heart is now functioning inside a fixed container.
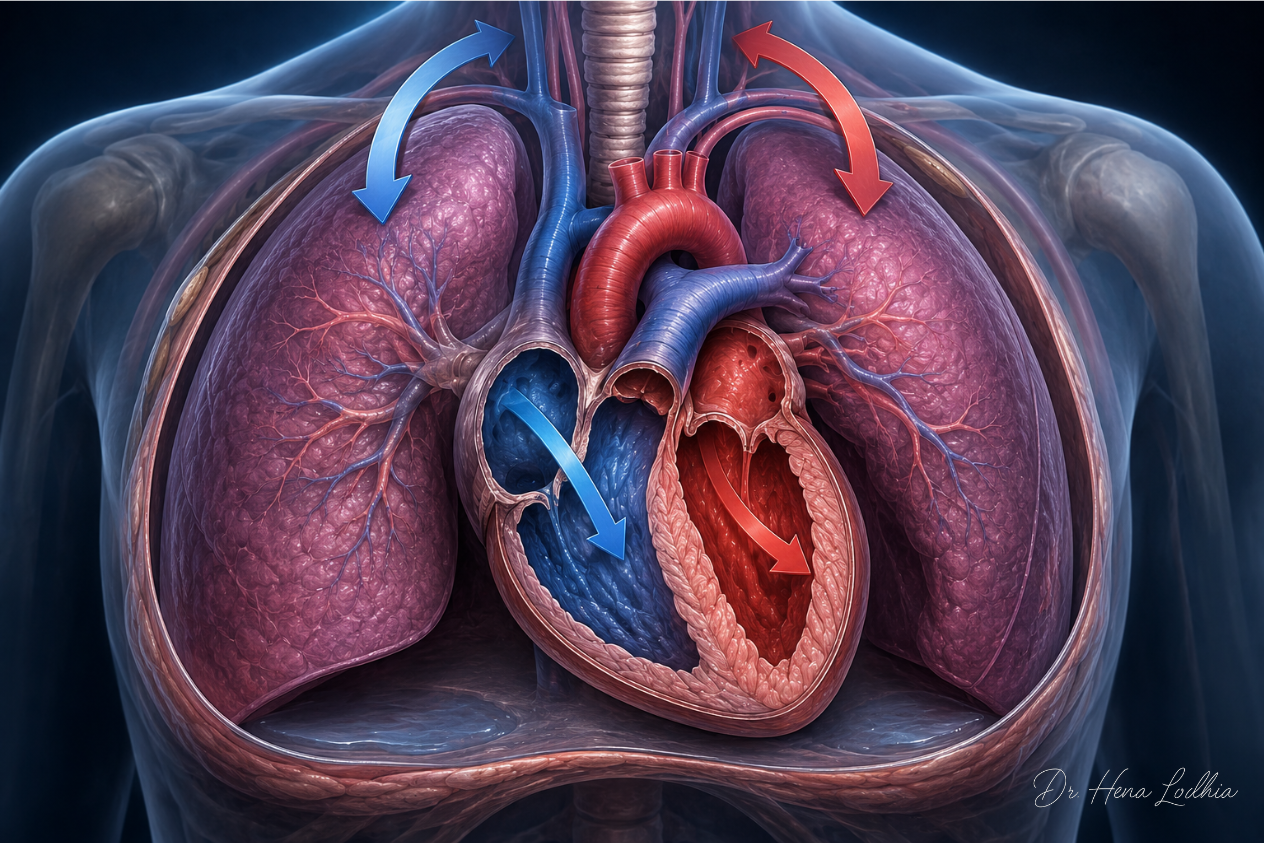
During inspiration, venous return to the right ventricle increases. In a normal heart, the right ventricle can expand outward. In tamponade, outward expansion is limited by elevated pericardial pressure.
The extra right-sided volume must be accommodated somewhere.
It is accommodated by shifting the interventricular septum toward the left ventricle.
That shift reduces left ventricular diastolic filling. Reduced left ventricular filling lowers stroke volume. Lower stroke volume lowers systolic pressure.
The chain is:
Spontaneous inspiration
↓
Increased systemic venous return to the right ventricle
↓
Right ventricle cannot expand outward because pericardial pressure is high
↓
Septum shifts leftward
↓
Left ventricular filling falls
↓
Left ventricular stroke volume falls
↓
Systolic pressure drops during inspiration
Pulmonary vascular pooling may contribute, but it is not the dominant mechanism. The dominant event in tamponade is exaggerated ventricular interdependence caused by pericardial constraint.
This is why echocardiography detects the same physiology visually: right atrial collapse, right ventricular diastolic collapse, plethoric inferior vena cava, and exaggerated respiratory variation in transvalvular flow.
The cuff finding and the ultrasound findings are different expressions of the same hemodynamic problem.
Constrictive Pericarditis: Fixed Volume Plus Pressure Dissociation
Constrictive pericarditis can resemble tamponade clinically, but the physiology is not identical.
In constriction, the pericardium becomes rigid because of fibrosis, calcification, inflammation, or scarring. The ventricles fill rapidly in early diastole and then stop abruptly when the fixed pericardial limit is reached.
The heart is again constrained, but constriction adds another mechanism: impaired transmission of intrathoracic pressure to the cardiac chambers.
During normal inspiration, intrathoracic pressure falls. This fall is transmitted to the pulmonary veins, left atrium, and left ventricle. Because these pressures fall together, the pressure gradient from pulmonary veins to left atrium is maintained.
In constrictive pericarditis, the rigid pericardium partially isolates the cardiac chambers from intrathoracic pressure changes. Pulmonary venous pressure falls with inspiration, but left atrial pressure does not fall proportionally.
The gradient from pulmonary veins to the left atrium decreases.
Left atrial filling falls. Left ventricular filling falls. Stroke volume falls.
At the same time, systemic venous return to the right ventricle increases during inspiration. Because the total cardiac volume is constrained, increased right-sided filling shifts the septum leftward and further reduces left ventricular filling.
So constriction produces respiratory variation through two linked mechanisms:
impaired transmission of intrathoracic pressure
+
exaggerated ventricular interdependence
This is why constriction should not be described simply as “chronic tamponade.” Both restrict diastolic filling, but their pressure relationships are different.
Severe Asthma and COPD: When Respiratory Effort Distorts Cardiac Loading
In severe obstructive airway disease, the primary problem is not a fixed pericardium.
The primary problem is extreme respiratory mechanics.
Bronchospasm, mucosal edema, mucus plugging, airway collapse, and dynamic hyperinflation force the patient to generate markedly negative intrathoracic pressures during inspiration.
Those pressure swings affect the heart in several ways.
First, markedly negative intrathoracic pressure increases systemic venous return to the right ventricle. Right ventricular filling rises. If right ventricular volume increases enough, the septum shifts toward the left ventricle and reduces left ventricular filling.
Second, negative intrathoracic pressure increases left ventricular transmural pressure.
Left ventricular transmural pressure is:
LV intracavitary pressure − intrathoracic pressure
When intrathoracic pressure becomes very negative, the pressure difference across the left ventricular wall increases. The left ventricle must generate more force to eject blood into the systemic circulation. Effective left ventricular afterload rises, even if cuff-measured arterial pressure has not changed.
Third, dynamic hyperinflation compresses pulmonary vessels. Pulmonary vascular resistance rises. The right ventricle faces increased afterload, dilates, and pushes the septum further toward the left ventricle.
The chain is:
Severe airway obstruction
↓
Large negative inspiratory intrathoracic pressure
↓
Increased venous return to the right ventricle
+
Increased LV transmural afterload
+
Dynamic hyperinflation with increased pulmonary vascular resistance
↓
Right ventricular dilation and septal shift
↓
Reduced LV filling and impaired LV ejection
↓
Exaggerated inspiratory fall in systolic pressure
This explains why pulsus paradoxus may be prominent in severe asthma.
It also explains a dangerous clinical trap. A large pulsus paradoxus can reflect severe respiratory effort. But if a deteriorating asthmatic patient develops respiratory muscle fatigue, the patient may no longer generate large negative intrathoracic pressures. Pulsus paradoxus may decrease because the patient is failing, not because the physiology has improved.
A disappearing pulsus paradoxus in a tiring asthmatic patient can therefore be ominous.
Massive Pulmonary Embolism: Acute Right Ventricular Pressure Overload
Massive pulmonary embolism can produce pulsus paradoxus through acute right ventricular pressure overload.
A large embolic burden abruptly increases pulmonary vascular resistance. The right ventricle, which is adapted to a low-pressure pulmonary circulation, suddenly faces a high afterload.
The right ventricle dilates. Septal position shifts leftward. Left ventricular diastolic filling decreases. Cardiac output falls.
The pericardium matters here as well. Acute right ventricular dilation occurs within a limited pericardial space. As the right ventricle enlarges, it reduces the space available for left ventricular filling.
During inspiration, increased venous return further loads the already strained right ventricle. Septal shift becomes more pronounced. Left ventricular filling falls further.
In massive pulmonary embolism, pulsus paradoxus is therefore not a primary pericardial sign. It reflects acute right ventricular pressure overload, pericardial limitation, and ventricular interdependence.
Tension Pneumothorax: Obstructive Shock Dominates
Tension pneumothorax may be associated with respiratory variation in arterial pressure, but it should not be forced into the same mechanism as tamponade.
The dominant event is rising intrapleural pressure.
Air enters the pleural space and cannot escape. Intrapleural pressure rises progressively. Venous return to the thorax falls. Mediastinal shift further compromises cardiac filling. Pulmonary blood flow decreases. Left ventricular preload falls. Cardiac output collapses.
Respiration can exaggerate these pressure changes, but pulsus paradoxus is not the central diagnostic concept in tension pneumothorax.
The key clinical issue is obstructive shock requiring immediate decompression.
Profound Hypovolemia: Preload Dependence Magnifies Normal Variation
Severe hypovolemia can exaggerate the inspiratory fall in systolic pressure because the ventricle becomes highly preload dependent.
When intravascular volume is markedly reduced, the left ventricle operates on the steep portion of the Frank-Starling curve. Small changes in filling produce large changes in stroke volume.
Normal respiration produces small fluctuations in venous return and left ventricular preload. In a euvolemic patient, these fluctuations have little effect. In profound hypovolemia, the same respiratory fluctuations can produce marked changes in stroke volume and systolic pressure.
The mechanism is not pericardial constraint.
It is extreme preload sensitivity.
Measurement: Useful Historically, Less Central Today
Formal measurement of pulsus paradoxus is straightforward in principle.
The cuff is inflated above systolic pressure and slowly deflated. The clinician identifies the pressure at which Korotkoff sounds are audible only during expiration. The cuff is then lowered until Korotkoff sounds are audible throughout the respiratory cycle.
The difference between these two pressures is the pulsus paradoxus.
A value greater than 10 mmHg is generally considered abnormal.
In real clinical practice, careful measurement may be difficult. Tachypnea, agitation, arrhythmias, weak pulses, noisy emergency settings, and urgent instability all reduce reliability.
That is why point-of-care ultrasound and echocardiography have largely displaced formal cuff measurement in suspected tamponade.
But modern imaging did not replace the physiology.
It simply made the physiology visible.
Common Misconceptions
Pulsus paradoxus does not mean the heart stops beating during inspiration.
It does not mean the central pulse truly disappears.
It is not specific for cardiac tamponade.
Its absence does not exclude tamponade.
Its presence does not prove tamponade.
It is not obsolete physiologically, even if it is less often measured formally.
It is not always reassuring when it decreases. In severe asthma, a falling pulsus paradoxus during clinical deterioration may indicate respiratory muscle fatigue.
The most important misconception is that pulsus paradoxus is a diagnosis. It is not. It is a hemodynamic pattern.
It tells the clinician that respiration is causing an abnormally large change in left ventricular output.
Clinical Pearls
Pulsus paradoxus is best understood as an exaggerated inspiratory reduction in left ventricular stroke volume.
In tamponade, the dominant mechanism is pericardial constraint causing exaggerated ventricular interdependence.
In constrictive pericarditis, the mechanism combines ventricular interdependence with impaired transmission of intrathoracic pressure to the cardiac chambers.
In severe asthma and COPD, the mechanism is driven by large negative intrathoracic pressure swings, increased LV transmural afterload, dynamic hyperinflation, increased pulmonary vascular resistance, and right ventricular strain.
In massive pulmonary embolism, the mechanism is acute right ventricular pressure overload within a limited pericardial space.
In profound hypovolemia, the mechanism is extreme preload dependence.
The formal bedside measurement of pulsus paradoxus is less central in modern practice because ultrasound can identify tamponade physiology more directly and quickly.
But the concept remains essential.
Pulsus paradoxus is not merely an old physical sign. It is a clinical expression of a deeper hemodynamic question:
Why is inspiration making the left ventricle eject less blood?
Answering that question explains not only the fading pulse, but also the physiology of tamponade, constriction, severe obstructive lung disease, massive pulmonary embolism, and other states where respiration and circulation become dangerously interdependent.
CLINICAL REFERENCES
- Hamzaoui O. Pulsus paradoxus. Eur Respir J. 2013;42(6):1696-1705. doi:10.1183/09031936.00138912
- Little WC, Freeman GL. Pericardial disease. Circulation. 2006;113(12):1622-1632. doi:10.1161/CIRCULATIONAHA.105.561514
- Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003;349(7):684-690. doi:10.1056/NEJMra022643
- Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015;36(42):2921-2964. doi:10.1093/eurheartj/ehv318
- Pérez-Casares A, Cesar S, Brunet-Garcia L, Sanchez-de-Toledo J. Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade. Front Pediatr. 2017;5:79. doi:10.3389/fped.2017.00079
- Petit M, Vieillard-Baron A, Evrard B. Ventricular interdependence in critically ill patients. Front Cardiovasc Med. 2023;10:1155981. doi:10.3389/fcvm.2023.1155981
- Sarkar M, Niranjan N, Banyal PK. Mechanisms of hypoxemia. Lung India. 2017;34(1):47-60. doi:10.4103/0970-2113.197116
- Maisch B, Seferović PM, Ristić AD, et al. Guidelines on the diagnosis and management of pericardial diseases. Executive summary. Eur Heart J. 2004;25(7):587-610. doi:10.1016/j.ehj.2004.02.002
- Reddy PS, Curtiss EI, Uretsky BF. Spectrum of hemodynamic changes in cardiac tamponade. Am J Cardiol. 1990;66(20):1487-1491. doi:10.1016/0002-9149(90)90540-g
- Guntheroth WG. Sensitivity and Specificity of Echocardiographic Evidence of Tamponade: Implications for Ventricular Interdependence and Pulsus Paradoxus. Pediatr Cardiol. 2008;29(4):758-762. doi:10.1007/s00246-008-9218-1
- Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF, editors. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 11th ed. Philadelphia, PA: Elsevier; 2019.
- Hall JE, Hall ME. Guyton and Hall Textbook of Medical Physiology. 14th ed. Philadelphia, PA: Elsevier; 2021.
References selected from peer-reviewed literature, major guidelines, and standard medical textbooks.

Educational Note
Medicine is more than memorising facts—it is understanding the physiological processes that connect symptoms, signs, investigations, and clinical outcomes.
This article is designed to help students, healthcare professionals, and curious learners develop deeper clinical reasoning by exploring the mechanisms behind disease. The goal is not only to improve examination performance but also to strengthen real-world diagnostic thinking and patient care.
Disclaimer
This content is provided for educational and informational purposes only. It is not intended to replace professional medical advice, diagnosis, or treatment.
Clinical decisions should always be based on individual patient evaluation, current evidence-based guidelines, institutional protocols, and professional judgment. While every effort has been made to ensure accuracy at the time of publication, medical knowledge continues to evolve, and readers should consult up-to-date references when making clinical decisions.
Go Deeper
Keeping up with medical research is difficult.
Thousands of new studies are published every year, yet most clinicians have limited time to read, analyze, and determine what truly matters for patient care.
Clinical Logic is a research-focused newsletter that breaks down important medical studies into clear, practical insights. Each edition translates complex research into plain language, highlighting what the findings mean, why they matter, and how they may influence clinical practice.
Whether you’re a student, resident, pharmacist, or practicing clinician, Clinical Logic helps you stay connected to the evolving world of medicine—without spending hours reading journals.