Why Does Asterixis Occur?
The Mechanism Behind the “Flapping” Hand
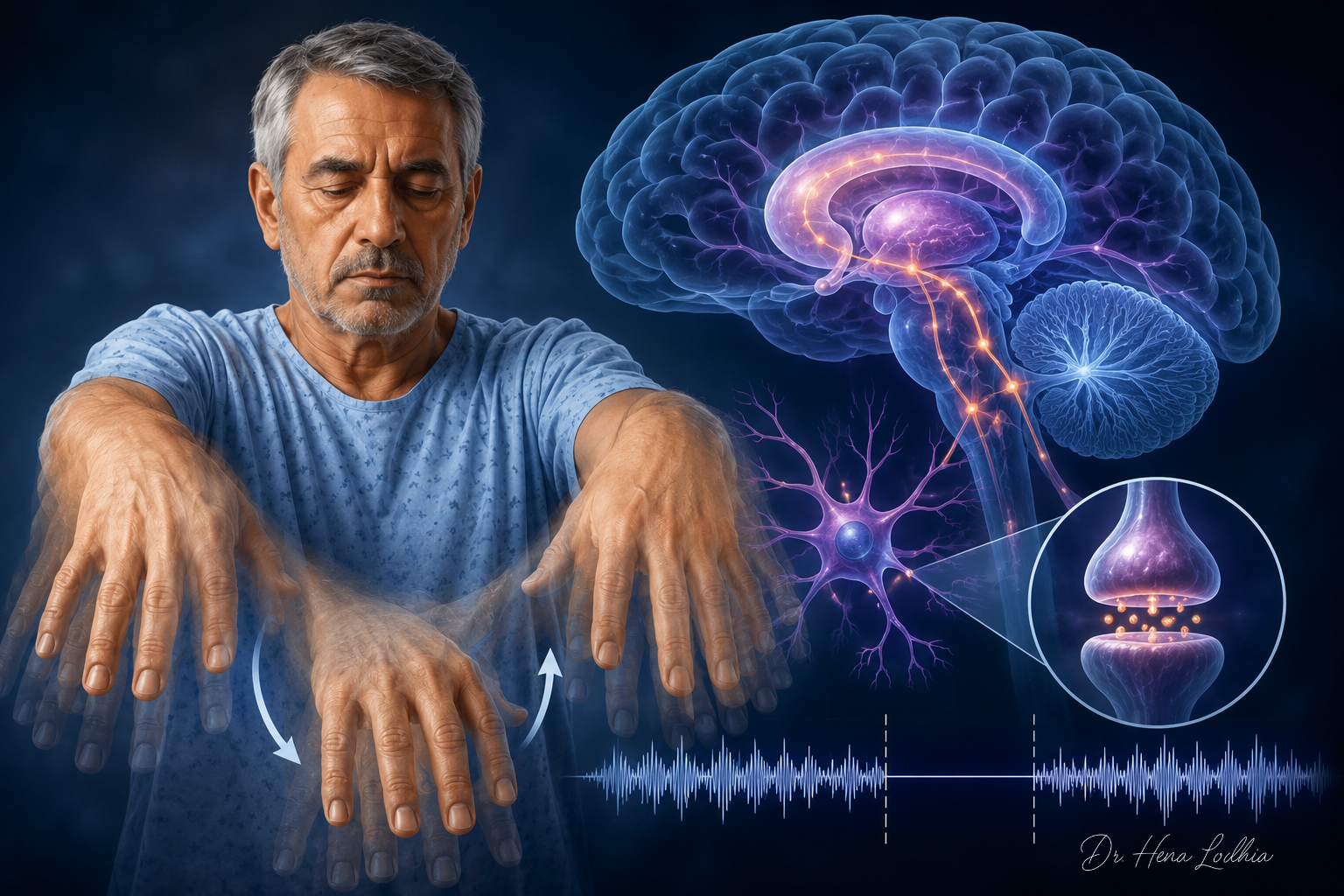
A 62-year-old man with decompensated cirrhosis is brought to the emergency department because his family says he has become slow, irritable, and unusually sleepy. He is mildly dehydrated and has not opened his bowels for several days. When asked to stretch out both arms, extend the wrists, and spread the fingers, he initially holds the posture. After a few seconds, both hands suddenly drop at the wrists and metacarpophalangeal joints, then rapidly return to extension. The movement is irregular, non-rhythmic, and more obvious when he tries to maintain the posture.
This is asterixis.
🎧 Clinical Summary Audio
Listen to the key concept in under 60 seconds.
It is often called a “flapping tremor,” but that phrase is misleading. A tremor is rhythmic. Asterixis is not. A tremor is produced by oscillating muscle activity. Asterixis is produced by a brief interruption of muscle activity. The hand appears to flap because the brain momentarily fails to maintain the motor command required to hold posture.
The Diagnostic Trap
The first trap is to localize the problem to the hand. The wrist drops, so the movement looks peripheral. But in typical bilateral asterixis, the wrist extensors are not primarily weak, the peripheral nerves are not the main lesion, and the neuromuscular junction is intact. The patient can usually initiate movement. The problem is sustaining posture.
The second trap is to treat asterixis as synonymous with hepatic encephalopathy. Hepatic encephalopathy is the classic association, but asterixis is not liver-specific. It can occur in uremia, hypercapnia, sedative toxicity, antiepileptic toxicity, lithium toxicity, severe electrolyte disturbance, sepsis-associated encephalopathy, Wilson disease, and focal structural brain lesions.
Raymond Adams and Joseph Foley described asterixis in 1949 in patients with hepatic encephalopathy. The older term “liver flap” helped clinicians recognize the sign, but it also narrowed the differential. Modern neurophysiology understands asterixis as negative myoclonus: a sudden, brief loss of ongoing muscle contraction during attempted sustained posture.
What Actually Fails?
Maintaining posture is an active neurological process. To keep the wrists extended, the brain must continuously activate agonist muscles while integrating proprioceptive feedback, gravitational load, attention, and corrective motor responses. This depends on coordinated activity across cortical motor areas, thalamocortical pathways, cerebellar output, basal ganglia modulation, brainstem pathways, spinal motor neurons, and sensory feedback loops.
In asterixis, these systems do not fail permanently. They fail intermittently.
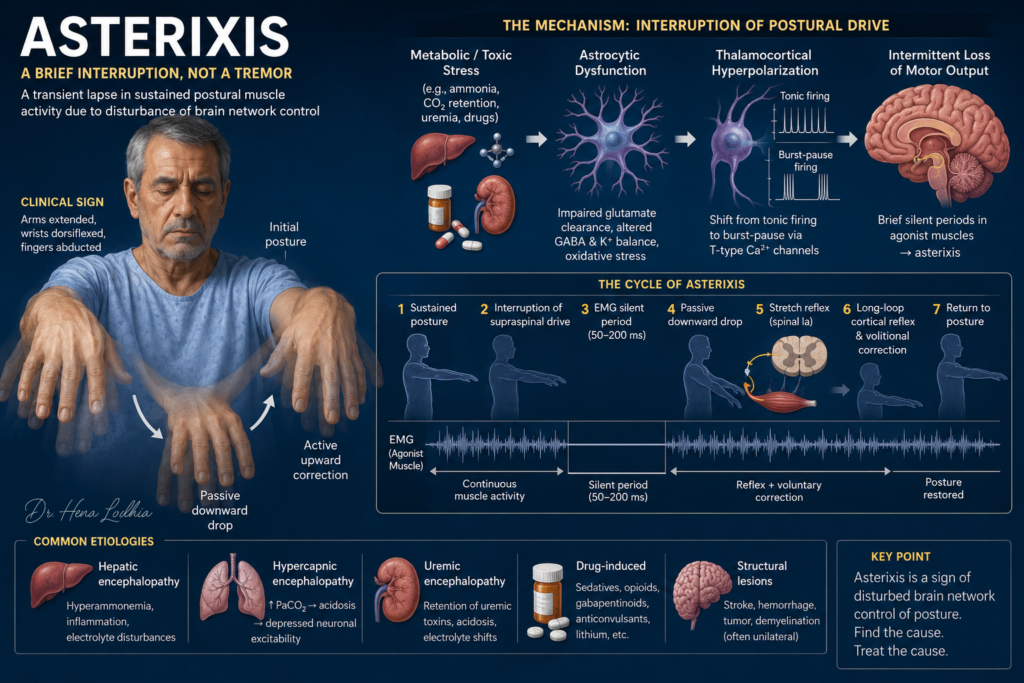
Electromyographic studies show brief silent periods in muscles that were previously contracting, often lasting approximately 50–200 milliseconds. During that silent period, the postural command is interrupted. Gravity pulls the hand downward. The return movement is active: first through stretch reflexes and then through renewed voluntary motor drive.
The sequence is:
Sustained posture
↓
Continuous agonist muscle activity
↓
Brief interruption of supraspinal motor drive
↓
Short EMG silent period
↓
Passive downward drop under gravity
↓
Reflex and voluntary correction
↓
Return to posture
This is why asterixis is irregular. A tremor is an added rhythmic movement. Asterixis is a brief subtraction from normal posture.
The Final Common Pathway
Asterixis is best understood as a network-level failure of sustained postural control. No single universal “asterixis center” has been identified. Metabolic, toxic, respiratory, pharmacological, and structural disorders can all disturb the motor-regulatory systems that keep posture stable.
The final common pathway is:
Brain dysfunction
↓
Impaired cortical-subcortical regulation of posture
↓
Intermittent loss of tonic muscle activity
↓
Negative myoclonus
↓
Asterixis
The key idea is simple but important: the hand does not flap because the brain sends an abnormal downward command. The hand drops because the normal command briefly disappears.
Hepatic Encephalopathy: The Classic Example
In cirrhosis or portosystemic shunting, gut-derived nitrogenous substances bypass effective hepatic detoxification. Ammonia is important, but it is not the whole explanation. Infection, gastrointestinal bleeding, constipation, renal dysfunction, dehydration, hyponatremia, hypokalemia, sedatives, and systemic inflammation all influence whether encephalopathy develops.
A more accurate chain is:
Cirrhosis or portosystemic shunting
↓
Reduced hepatic clearance of ammonia and other gut-derived neurotoxins
↓
Increased neurotoxin delivery to the brain
↓
Astrocytic ammonia detoxification through glutamine synthesis
↓
Glutamine accumulation, osmotic stress, mitochondrial dysfunction, and oxidative stress
↓
Impaired regulation of glutamate, extracellular potassium, water balance, and synaptic stability
↓
Disturbed cortical-subcortical motor regulation
↓
Intermittent failure of sustained postural drive
↓
Asterixis
This explains why serum ammonia does not perfectly correlate with clinical severity. Ammonia contributes, but the bedside sign reflects the combined burden of glial dysfunction, inflammation, cerebral reserve, shunting, and precipitating illness.
Why Astrocytes Matter
Astrocytes are central to hepatic encephalopathy because they regulate the chemical environment in which neurons function. They clear glutamate, buffer extracellular potassium, participate in ammonia detoxification, maintain osmotic balance, and support synaptic signaling. When astrocytes are metabolically stressed, neuronal communication becomes less reliable.
This is why asterixis often appears with impaired attention, psychomotor slowing, sleep-wake reversal, and disorientation. The motor sign and the mental status change are not separate phenomena. Both reflect disturbed brain network function.
Hypercapnia: When CO₂ Depresses Motor Control
In COPD exacerbation, obesity hypoventilation, neuromuscular ventilatory failure, or sedative-induced hypoventilation, carbon dioxide accumulates. CO₂ crosses the blood-brain barrier rapidly and lowers cerebrospinal fluid pH. The resulting acidosis depresses neuronal responsiveness and impairs cortical-subcortical motor coordination.
The chain is:
Alveolar hypoventilation
↓
Rising PaCO₂
↓
Cerebrospinal fluid acidosis
↓
Depressed neuronal responsiveness
↓
Brief lapses in sustained postural output
↓
Asterixis
In a drowsy patient with chronic lung disease, asterixis should raise concern for CO₂ retention. It may be a bedside warning of hypercapnic respiratory failure.
Uremic Encephalopathy
In renal failure, retained uremic solutes, acidosis, electrolyte disturbance, inflammation, hypertension, and drug accumulation can impair neuronal and glial function. These disturbances alter synaptic signaling across motor-regulatory circuits.
Clinically, uremic encephalopathy may produce confusion, myoclonus, seizures, and asterixis. In advanced kidney disease, asterixis is not merely a neurological curiosity. It may signal clinically significant uremia and influence the urgency of renal replacement therapy.
Drug-Induced Asterixis
Drug-induced asterixis is frequently missed because the movement is attributed to “metabolic encephalopathy” without reviewing the medication list. Common culprits include benzodiazepines, barbiturates, opioids, gabapentin, pregabalin, baclofen, lithium, phenytoin, carbamazepine, and valproate.
The mechanism varies. Sedatives and opioids depress cortical responsiveness. Gabapentinoids and baclofen may accumulate in renal impairment. Lithium can disturb neuronal excitability. Antiepileptics can impair motor network timing through dose-related neurotoxicity.
Valproate deserves special attention. Valproate-induced hyperammonemic encephalopathy can occur even when liver enzymes are normal. A patient on valproate who develops confusion and asterixis needs serum ammonia and valproate level assessment, not reassurance from a normal hepatic panel alone.
Why Asterixis Is Usually Bilateral but Can Be Unilateral
Bilateral asterixis usually points toward diffuse metabolic, toxic, respiratory, renal, hepatic, septic, or drug-related brain dysfunction. Both hemispheres and their motor-regulatory networks are affected, so the sign appears on both sides, though often asymmetrically.
Unilateral asterixis suggests a focal structural lesion interrupting motor-control networks on one side. Lesions may involve the contralateral thalamus, internal capsule, parietal cortex, or other supratentorial motor-regulatory areas. Brainstem or midbrain lesions may produce ipsilateral asterixis depending on the level and pathway involved.
This distinction matters. Bilateral asterixis should trigger metabolic, respiratory, renal, hepatic, infectious, and medication evaluation. New unilateral asterixis should prompt neuroimaging to exclude stroke, hemorrhage, tumor, demyelination, or another focal lesion.
Bedside Examination Beyond the Hands
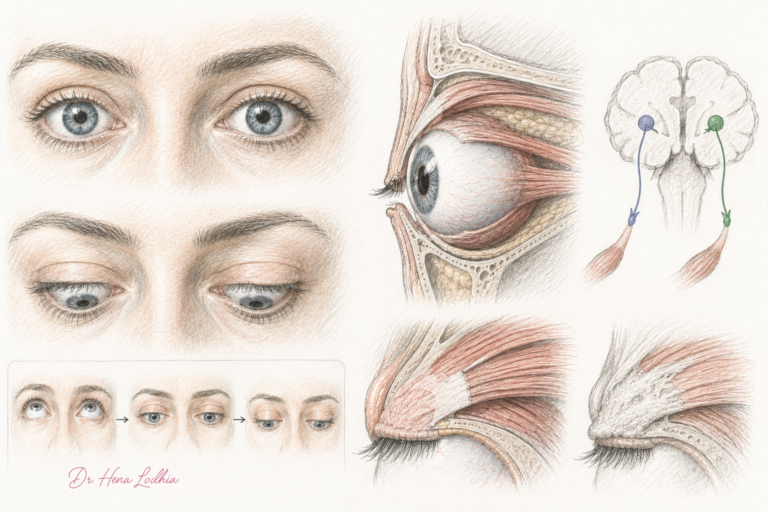
The classic maneuver is to ask the patient to extend both arms, dorsiflex the wrists, and spread the fingers. The examiner should look for irregular lapses rather than rhythmic oscillation. Asking the patient to close the eyes may make the sign more apparent.
Asterixis can also be elicited outside the upper limbs. It may appear with tongue protrusion, eyelid closure, or lower-limb posturing. In the legs, it may be seen when the hips and knees are flexed or when the feet are dorsiflexed against gravity. These variants reinforce the central concept: asterixis is a disorder of sustained posture, not a disease of the wrist.
Why Severe Encephalopathy May Have Less Asterixis
A common misconception is that more encephalopathy always means more asterixis. This is not true.
Asterixis requires the patient to attempt and briefly maintain a posture. In mild to moderate encephalopathy, the patient can cooperate enough for intermittent lapses to become visible. In profound encephalopathy, stupor, coma, severe inattention, or inability to follow commands may prevent sustained posture altogether. The sign may become difficult to elicit or disappear, not because the brain has improved, but because the patient can no longer generate the baseline posture required to reveal the negative myoclonus.
This is clinically important in hepatic encephalopathy. Asterixis is often associated with overt encephalopathy, especially around grade II, but its absence does not exclude severe disease.
Common Misconceptions
The phrase “flapping tremor” describes the appearance but not the physiology. Asterixis is negative myoclonus, not a true tremor.
Asterixis is not pathognomonic for hepatic encephalopathy. It is a sign of impaired brain network function and must be interpreted in clinical context.
Asterixis is not weakness. Strength may be normal on brief testing. The abnormality appears when the patient is asked to sustain posture.
Ammonia is not the whole story in hepatic encephalopathy. Clinical expression depends on inflammation, renal function, electrolyte status, medications, shunting, cerebral reserve, and precipitating illness.
Absence of asterixis does not exclude encephalopathy, especially if the patient is too drowsy, uncooperative, or comatose to maintain posture.
Clinical Implications
Asterixis should immediately change the diagnostic question from “Why is the hand shaking?” to “What is interrupting this patient’s sustained supraspinal motor output?”
In a patient with cirrhosis, that means searching for gastrointestinal bleeding, constipation, infection, spontaneous bacterial peritonitis, dehydration, renal impairment, hypokalemia, hyponatremia, overdiuresis, sedatives, opioids, and recent medication changes. Treating hepatic encephalopathy with lactulose or rifaximin without identifying the precipitant is incomplete care.
In a patient with chronic lung disease, asterixis may be an early bedside clue to hypercapnic respiratory failure.
In renal failure, it may indicate clinically important uremic encephalopathy.
In hospitalized older adults, it may reveal drug accumulation or sedative burden before the medication list has been fully appreciated.
In unilateral asterixis, the priority shifts toward focal neurological localization and urgent brain imaging.
Key Clinical Pearls
Asterixis is negative myoclonus: a brief interruption of ongoing muscle contraction.
The EMG signature is a short silent period in an actively contracting muscle.
The downward flap is passive; the return is active correction.
Bilateral asterixis usually suggests diffuse metabolic, toxic, respiratory, renal, hepatic, septic, or drug-related encephalopathy.
Unilateral asterixis suggests a focal structural lesion until proven otherwise.
Valproate-induced hyperammonemic encephalopathy can occur with normal liver enzymes.
Asterixis may disappear in very severe encephalopathy because the patient can no longer sustain the posture needed to demonstrate it.
Final Clinical Takeaway
Asterixis occurs because the brain briefly fails to maintain continuous postural motor output.
The visible flap is not an added movement. It is the temporary absence of a normal command, followed by reflex and voluntary correction. Whether the cause is hepatic encephalopathy, CO₂ retention, uremia, drug toxicity, electrolyte disturbance, sepsis, or a focal lesion, the bedside sign points to impaired network-level control of posture.
That is why asterixis remains valuable. It converts a vague presentation such as confusion, drowsiness, or “shaking” into a focused search for reversible brain dysfunction.
CLINICAL REFERENCES
- Adams RD, Foley JM. The neurological changes in the more common types of severe liver disease. Transactions of the American Neurological Association. 1949.
- Leavitt S, Tyler HR. Studies in Asterixis. Part I. Archives of Neurology. 1964.
- Caviness JN. Negative myoclonus: An overview of its clinical features, neurophysiology, and treatment. Neurophysiologie Clinique / Clinical Neurophysiology. 2007.
- Vilstrup H, Amodio P, Bajaj J, et al. Hepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guideline by AASLD and EASL. Hepatology. 2014. doi: 10.1002/hep.27210.
- Zackria R. Asterixis. StatPearls Publishing. 2024.
FURTHER READING
- Rissardo JP, Fornari ACL, Caprara ALF. Flapping Tremor: Unraveling Asterixis—A Narrative Review. Medicina (Kaunas). 2024. doi: 10.3390/medicina60030362.
- Shibasaki H. Pathophysiology of Negative Myoclonus and Asterixis. Advances in Neurology, Volume 67: Negative Motor Phenomena. 1995.
- Young RR, Shahani BT. Asterixis: One Type of Negative Myoclonus. Advances in Neurology, Volume 43: Myoclonus. 1986.
- Conn HO, Lieberthal MM. Asterixis: Its Occurrence in Chronic Pulmonary Disease and Respiratory Failure. New England Journal of Medicine. 1958.
- Mullen KD. Review of the Final Report of the 1998 Working Party on Hepatic Encephalopathy. Alimentary Pharmacology & Therapeutics. 2007. doi: 10.1111/j.1365-2036.2006.02942.x.
- Chandarana M, et al. Myoclonus: A Review. Annals of Indian Academy of Neurology. 2021.
- Ficker DM, et al. Cortical Activation Associated with Asterixis in Manifest Hepatic Encephalopathy. Acta Neurologica Scandinavica. 2014.
- Lanska DJ. Raymond D. Adams and Joseph M. Foley: Elaborating the Neurologic Manifestations of Hepatic Encephalopathy (1949–1953). Journal of the History of the Neurosciences. 2021. doi: 10.1080/0964704X.2021.1891691.
References selected from peer-reviewed literature, major guidelines, and standard medical textbooks.

Educational Note
Medicine is more than memorising facts—it is understanding the physiological processes that connect symptoms, signs, investigations, and clinical outcomes.
This article is designed to help students, healthcare professionals, and curious learners develop deeper clinical reasoning by exploring the mechanisms behind disease. The goal is not only to improve examination performance but also to strengthen real-world diagnostic thinking and patient care.
Disclaimer
This content is provided for educational and informational purposes only. It is not intended to replace professional medical advice, diagnosis, or treatment.
Clinical decisions should always be based on individual patient evaluation, current evidence-based guidelines, institutional protocols, and professional judgment. While every effort has been made to ensure accuracy at the time of publication, medical knowledge continues to evolve, and readers should consult up-to-date references when making clinical decisions.
Go Deeper
Keeping up with medical research is difficult.
Thousands of new studies are published every year, yet most clinicians have limited time to read, analyze, and determine what truly matters for patient care.
Clinical Logic is a research-focused newsletter that breaks down important medical studies into clear, practical insights. Each edition translates complex research into plain language, highlighting what the findings mean, why they matter, and how they may influence clinical practice.
Whether you’re a student, resident, pharmacist, or practicing clinician, Clinical Logic helps you stay connected to the evolving world of medicine—without spending hours reading journals.