Why Does Lid Lag Occur?
Pathophysiology Behind Von Graefe Sign
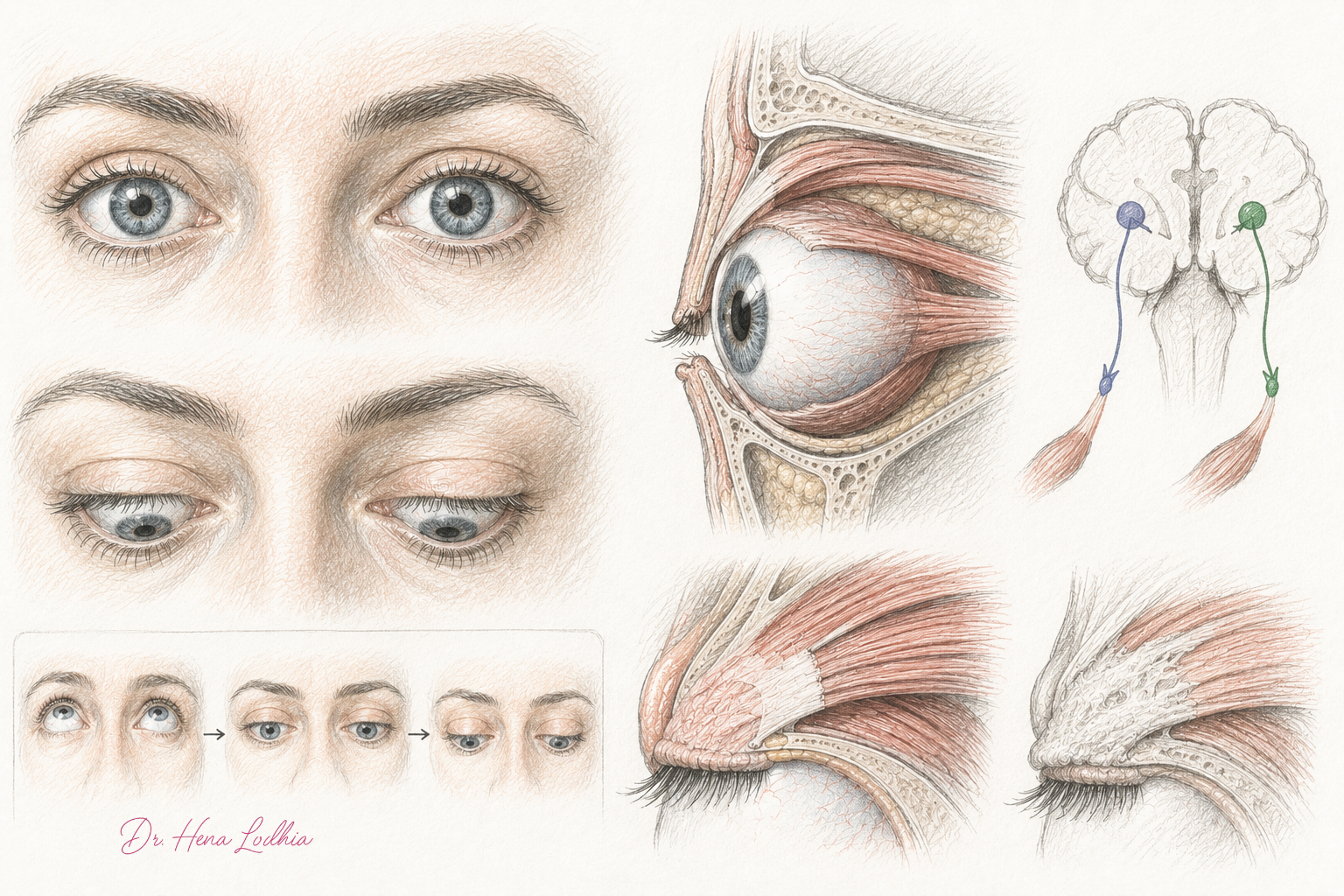
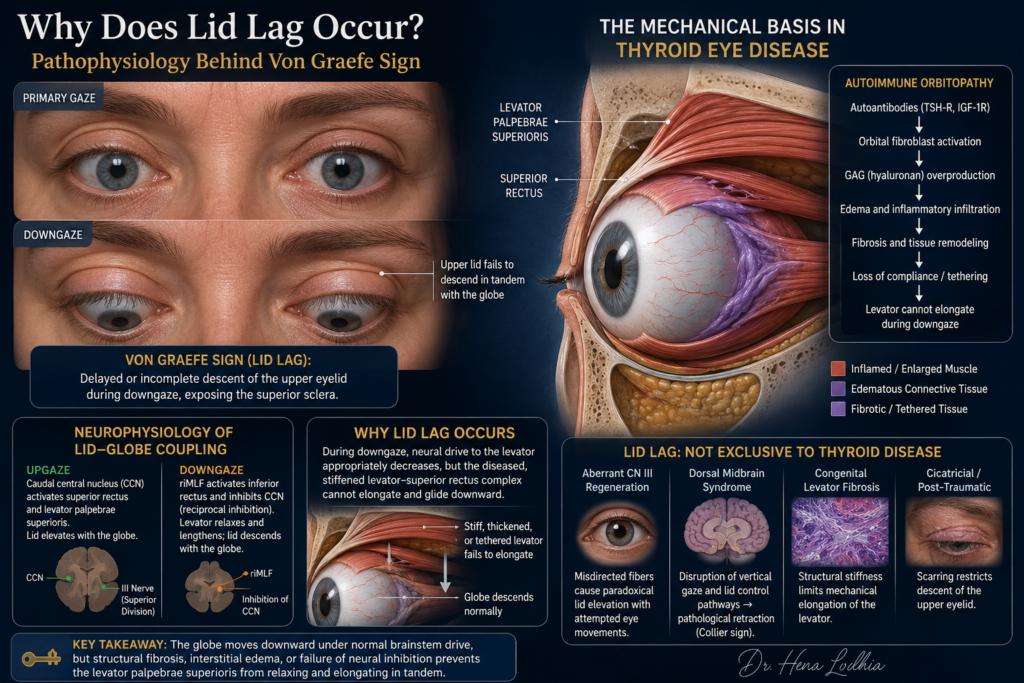
A patient with tremor, weight loss, heat intolerance, and palpitations is asked to follow the examiner’s finger from upgaze into downgaze. The globes move downward, but the upper eyelids do not descend at the same pace. For a brief moment, a band of superior sclera remains visible between the upper lid margin and the corneal limbus.
🎧 Clinical Summary Audio
Listen to the key concept in under 60 seconds.
This is lid lag, classically called Von Graefe sign when seen in thyroid eye disease.
The finding is easy to recognize but often poorly understood. It is not simply a “thyroid stare.” It is not the same as proptosis. It is not explained completely by excess thyroid hormone. Lid lag is a dynamic failure of the upper eyelid to maintain normal movement coupling with the descending globe.
The Diagnostic Trap
Three ocular signs are frequently merged into one vague phrase: “prominent eyes.” They should be separated.
Lid retraction is a static sign. The upper eyelid rests too high in primary gaze.
Proptosis is an orbital volume sign. The globe is displaced forward because enlarged muscles, expanded orbital fat, and edematous soft tissue occupy more space within the rigid bony orbit.
Lid lag is a dynamic sign. It is elicited during downgaze: the globe descends, but the upper lid hesitates or descends incompletely.
The distinction matters because each sign points to a different mechanism. Proptosis asks us to think about orbital crowding. Lid retraction asks us to think about eyelid resting tone and structural shortening. Lid lag asks a more precise question: why does the upper eyelid fail to release and descend when the eye moves down?
Historical Context: Why the Sympathetic Explanation Persisted
Von Graefe sign became one of the classic bedside signs of Graves disease long before modern orbital imaging, immunopathology, or fibroblast biology were available. Early clinicians saw a patient with thyrotoxicosis, tremor, tachycardia, staring eyes, and lid signs. It was logical to attribute the ocular appearance to excessive sympathetic activity.
That older explanation is not entirely wrong. Thyrotoxicosis increases adrenergic responsiveness, and the sympathetically innervated Müller muscle can raise the upper lid slightly. This contributes to the wide-eyed appearance and to resting lid retraction.
But the sympathetic explanation is incomplete. Müller muscle is a smooth muscle that provides only a small amount of tonic eyelid elevation. It is not the main muscle responsible for rapid, coordinated upper lid tracking during vertical gaze. That role belongs primarily to the striated levator palpebrae superioris and its anatomical-functional relationship with the superior rectus.
The historical error was treating the “stare” and the “lag” as the same phenomenon. They overlap clinically, but they are not mechanically identical.
Normal Eyelid–Globe Coordination
In normal vertical gaze, the upper eyelid does not simply fall passively. Its position is actively coordinated with globe movement.
The levator palpebrae superioris is the principal elevator of the upper eyelid. It is closely linked to the superior rectus by embryological origin, fascial relationships, and shared innervation through the superior division of the oculomotor nerve. Functionally, the levator and superior rectus behave as a coordinated elevator complex: when the eye looks up, the lid must elevate; when the eye looks down, the lid must relax and descend.
During upgaze, increased activity in the vertical gaze system drives superior rectus contraction and levator activation. During downgaze, that levator drive must fall. The levator muscle and its aponeurotic-fascial attachments must then lengthen smoothly so that the lid margin travels downward with the cornea.
This is where lid lag occurs. The globe descends under appropriate gaze command, but the upper eyelid elevator apparatus fails to relax, elongate, or glide at the required speed. The sclera becomes visible not because the globe is moving abnormally fast, but because the lid is mechanically or neurologically delayed.
The Core Mechanism
The essential mechanism can be stated in one sentence:
Lid lag occurs when the globe descends but the levator-superior rectus eyelid complex fails to release and lengthen in synchrony.
That failure may be caused by structural stiffness, inflammatory edema, fibrosis, abnormal fascial tethering, persistent levator overactivity, or disordered neural inhibition. In Graves disease, the dominant mechanism is usually not primary brainstem disease but thyroid-associated orbital remodeling involving the levator-superior rectus complex and surrounding connective tissues.
This distinction is important. Neuroanatomy explains how normal eyelid movement should be coordinated. Orbital pathology explains why that coordination fails mechanically in most patients with thyroid eye disease.
Why Graves Disease Produces Lid Lag
Graves disease can affect the eyelid through two overlapping but unequal mechanisms: a functional adrenergic component and a structural autoimmune orbital component.
The functional component comes from thyrotoxicosis. Increased adrenergic sensitivity enhances Müller muscle tone and raises the upper eyelid slightly. This creates resting lid retraction and makes any dynamic lag more visible during downgaze. However, it does not fully explain persistent or marked lid lag, especially when the eye disease continues after thyroid hormone levels normalize.
The structural component is thyroid eye disease. Orbital fibroblasts expressing TSH receptors and IGF-1 receptors become activated by autoimmunity, cytokine signaling, and immune-cell interactions. These fibroblasts produce hydrophilic glycosaminoglycans, especially hyaluronan, which draw water into orbital tissues. The result is interstitial edema, inflammatory infiltration, extraocular muscle enlargement, expansion of orbital fat, and later collagen deposition.
When this process involves the levator palpebrae superioris, superior rectus, and their shared fascial attachments, the upper eyelid loses normal compliance. In the active phase, edema and inflammation thicken the tissues. In the chronic phase, fibrosis and shortening make them less elastic. During downgaze, neural drive to the levator may appropriately decrease, but the stiffened levator-aponeurotic complex cannot lengthen smoothly. The lid remains suspended while the globe moves down.
This is the mechanical heart of Graves-related lid lag.
Why the Levator-Superior Rectus Complex Matters
The levator should not be imagined as an isolated eyelid string. It sits in close anatomical relationship with the superior rectus. Fascial connections between the two structures help coordinate upper lid position with vertical globe movement.
In thyroid eye disease, inflammation rarely respects neat anatomical boundaries. Enlargement and remodeling of the superior rectus-levator complex can alter both eye movement and eyelid movement. The eyelid may sit higher at rest because of retraction, and it may descend poorly because the same tissue complex has become thickened, shortened, or tethered.
This explains why lid lag is often seen with other orbital signs: restricted ocular motility, vertical diplopia, proptosis, conjunctival congestion, chemosis, and exposure symptoms. They are not separate curiosities. They are different visible expressions of the same confined orbital disease process.
The Role of Brainstem Physiology
The brainstem still matters, but its role should be framed carefully.
Normal vertical gaze depends on supranuclear gaze centers, the oculomotor nuclei, and reciprocal patterns of activation and inhibition. During upgaze, levator activity rises with superior rectus activity. During downgaze, levator activity must be reduced so the lid can descend. This is consistent with the broader principle of reciprocal innervation: muscles that elevate must relax when the opposite movement is required.
In Graves disease, the problem is usually not that the brainstem cannot send the correct command. The problem is that the diseased eyelid-orbital tissues may not obey the command normally. A fibrotic levator complex cannot elongate just because neural firing has decreased.
In contrast, supranuclear disorders can produce lid abnormalities by a more primary neural mechanism. Dorsal midbrain syndromes, including Parinaud syndrome, may produce pathological lid retraction known as Collier sign, partly because vertical gaze and eyelid control pathways are disrupted. This is why lid lag should be localized anatomically rather than reflexively labeled as Graves disease.
The Inferior Rectus: Contributor, Not Main Cause
The inferior rectus is commonly involved in thyroid eye disease and often becomes enlarged, inflamed, and fibrotic. Its classic clinical effect is restricted upgaze with vertical diplopia.
Inferior rectus restriction does not directly pull the upper lid upward. Its contribution to lid lag is indirect. When upgaze is restricted, the central nervous system may increase elevator drive in an attempt to overcome the mechanical tether. Because superior rectus activation is linked with levator activation, this increased drive can exaggerate upper lid elevation and make subsequent downgaze lag more obvious.
This mechanism should not be overstated. Direct involvement of the levator-superior rectus complex remains the more central explanation for Graves-related lid lag. Inferior rectus restriction is better understood as an amplifier of abnormal vertical gaze-lid mechanics, not the primary cause in most cases.
Non-Thyroid Causes of Lid Lag
Lid lag is a sign, not a diagnosis. Any disorder that prevents the upper lid from descending normally with the globe can produce a similar clinical appearance.
In aberrant regeneration after third nerve palsy, misdirected regenerating fibers may innervate the levator abnormally. Attempted eye movement can then cause paradoxical lid elevation or impaired lid descent.
In dorsal midbrain syndrome, lesions near the posterior commissure and pretectal region disrupt vertical gaze and eyelid control pathways. The result may include upgaze palsy, convergence-retraction nystagmus, light-near dissociation, and pathological lid retraction or abnormal lid tracking.
In congenital levator fibrosis, the levator is structurally stiff from development. The lid cannot move through its normal excursion because the tissue itself lacks compliance.
In cicatricial eyelid disease, trauma, surgery, inflammation, or scarring can mechanically restrict lid descent. Here the problem is not thyroid hormone, autoimmunity, or brainstem control; it is a scarred eyelid that cannot glide.
These causes reinforce the central principle: lid lag occurs when eyelid descent is uncoupled from globe descent.
Common Misconceptions
The first misconception is that lid lag equals proptosis. Proptosis is forward globe displacement; lid lag is delayed upper lid descent during downgaze. They often coexist in Graves disease but do not describe the same anatomical problem.
The second misconception is that excess thyroid hormone alone causes lid lag. Thyrotoxicosis can exaggerate lid retraction through adrenergic effects, but persistent lid lag usually reflects structural orbital disease, especially involvement of the levator-superior rectus complex.
The third misconception is that a euthyroid patient cannot have thyroid eye disease. Thyroid eye disease may remain active after thyroid hormone levels are controlled and may occasionally present in euthyroid or hypothyroid states.
The fourth misconception is that lid lag is merely cosmetic. It may signal a disease process that threatens the cornea through exposure or the optic nerve through orbital apex crowding.
Why This Matters Clinically
When lid lag is seen, the examination should move beyond thyroid function tests. The clinician should assess the eye itself.
Visual acuity and color vision screen for optic nerve compromise. Pupils should be examined for a relative afferent pupillary defect. Ocular motility should be tested for restrictive diplopia. The cornea should be inspected for exposure keratopathy. The conjunctiva should be assessed for injection or chemosis. Proptosis should be measured when possible, and pain with eye movement should raise concern for active inflammation.
The most serious complications are exposure keratopathy and compressive optic neuropathy. Exposure keratopathy develops when lid retraction, lid lag, lagophthalmos, proptosis, and impaired blinking destabilize the tear film and leave the cornea unprotected. Compressive optic neuropathy occurs when enlarged extraocular muscles and swollen orbital tissues crowd the orbital apex and compromise optic nerve function.
Red flags include reduced visual acuity, new dyschromatopsia, relative afferent pupillary defect, progressive diplopia, corneal epithelial defect, severe orbital pain, or rapidly worsening proptosis. These findings require urgent ophthalmologic evaluation.
Treatment Implications
Treatment depends on whether the dominant process is functional retraction, active inflammation, or fixed fibrosis.
Restoring euthyroidism may reduce adrenergic lid retraction, but it may not reverse established lid lag if the levator-superior rectus complex has become fibrotic. This is why “thyroid numbers are normal” does not always mean the eye disease is controlled.
Mild disease is managed with lubrication, ocular surface protection, smoking cessation, and careful follow-up. Smoking is the most important modifiable risk factor; it increases the risk and severity of thyroid eye disease and worsens treatment response.
Active moderate-to-severe thyroid eye disease may require systemic immunomodulatory therapy. Intravenous glucocorticoids remain an important treatment in many protocols. Teprotumumab, an IGF-1 receptor antagonist, has changed the treatment landscape in selected patients by targeting a pathway central to orbital fibroblast activation. Its clinical effect supports the importance of IGF-1R-mediated fibroblast signaling, although thyroid eye disease is not reducible to one pathway alone.
Chronic inactive disease with fixed structural abnormalities is managed surgically when needed. The usual rehabilitative sequence is orbital decompression first, strabismus surgery second, and eyelid surgery last, because changing orbital volume or eye position can alter eyelid position.
Key Clinical Pearls
Lid lag is a dynamic sign: delayed descent of the upper eyelid during downgaze.
Von Graefe sign is the classic thyroid-associated form of lid lag.
Lid retraction is static. Proptosis is forward globe displacement. Lid lag is failure of eyelid tracking.
Müller muscle contributes mainly to resting lid retraction; it does not fully explain dynamic lid lag.
In Graves disease, persistent lid lag is best explained by disease of the levator-superior rectus complex: edema, inflammation, fibrosis, tethering, and loss of compliance.
Brainstem physiology explains normal eyelid-globe coordination; orbital disease usually explains why this coordination fails in thyroid eye disease.
Inferior rectus restriction can amplify abnormal lid mechanics but should not be treated as the main cause of lid lag.
A euthyroid state does not exclude active thyroid eye disease.
The bedside summary is simple:
The globe descends, but the upper eyelid elevator complex cannot release and lengthen in time.
CLINICAL REFERENCES
- Smith TJ, Hegedüs L. Graves’ Disease. N Engl J Med. 2016;375(16):1552-1565. doi:10.1056/NEJMra1510030
- Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ Orbitopathy (EUGOGO) Clinical Practice Guidelines for the Medical Management of Graves’ Orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479
- Burch HB, Perros P, Bednarczuk T, et al. Management of Thyroid Eye Disease: A Consensus Statement by the American Thyroid Association and the European Thyroid Association. Thyroid. 2022;32(12):1439-1470. doi:10.1089/thy.2022.0251
- Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the Treatment of Active Thyroid Eye Disease. N Engl J Med. 2020;382(4):341-352. doi:10.1056/NEJMoa1910434
- Rundle FF, Wilson CW. Development and Course of Exophthalmos and Ophthalmoplegia in Graves’ Disease with Special Reference to the Effect of Thyroidectomy. Clin Sci (Lond). 1945;5(3-4):177-194. PMID:21011831
FURTHER READING
- Bartalena L, Baldeschi L, Boboridis K, et al. The 2016 European Thyroid Association / European Group on Graves’ Orbitopathy Guidelines for the Management of Graves’ Orbitopathy. Eur Thyroid J. 2016;5(1):9-26. doi:10.1159/000443828
- Bartalena L, Baldeschi L, Dickinson AJ, et al. Consensus Statement of the European Group on Graves’ Orbitopathy (EUGOGO) on Management of Graves’ Orbitopathy. Eur J Endocrinol. 2008;158(3):273-285. doi:10.1530/EJE-07-0666
- Elia G, Fallahi P, Ragusa F, et al. Precision Medicine in Graves’ Disease and Ophthalmopathy. Front Pharmacol. 2021;12:754386. doi:10.3389/fphar.2021.754386
- Moledina M, Damato EM, Lee V. The Changing Landscape of Thyroid Eye Disease: Current Clinical Advances and Future Outlook. Eye. 2024;38(8):1425-1437. doi:10.1038/s41433-024-02967-9
- Bartalena L. Role of Teprotumumab in the Treatment of Active Moderate-to-Severe Graves’ Orbitopathy. Eur Thyroid J. 2022;11(6):e220185. doi:10.1530/ETJ-22-0185
References selected from peer-reviewed literature, major guidelines, and standard medical textbooks.

Educational Note
Medicine is more than memorising facts—it is understanding the physiological processes that connect symptoms, signs, investigations, and clinical outcomes.
This article is designed to help students, healthcare professionals, and curious learners develop deeper clinical reasoning by exploring the mechanisms behind disease. The goal is not only to improve examination performance but also to strengthen real-world diagnostic thinking and patient care.
Disclaimer
This content is provided for educational and informational purposes only. It is not intended to replace professional medical advice, diagnosis, or treatment.
Clinical decisions should always be based on individual patient evaluation, current evidence-based guidelines, institutional protocols, and professional judgment. While every effort has been made to ensure accuracy at the time of publication, medical knowledge continues to evolve, and readers should consult up-to-date references when making clinical decisions.
Go Deeper
Keeping up with medical research is difficult.
Thousands of new studies are published every year, yet most clinicians have limited time to read, analyze, and determine what truly matters for patient care.
Clinical Logic is a research-focused newsletter that breaks down important medical studies into clear, practical insights. Each edition translates complex research into plain language, highlighting what the findings mean, why they matter, and how they may influence clinical practice.
Whether you’re a student, resident, pharmacist, or practicing clinician, Clinical Logic helps you stay connected to the evolving world of medicine—without spending hours reading journals.