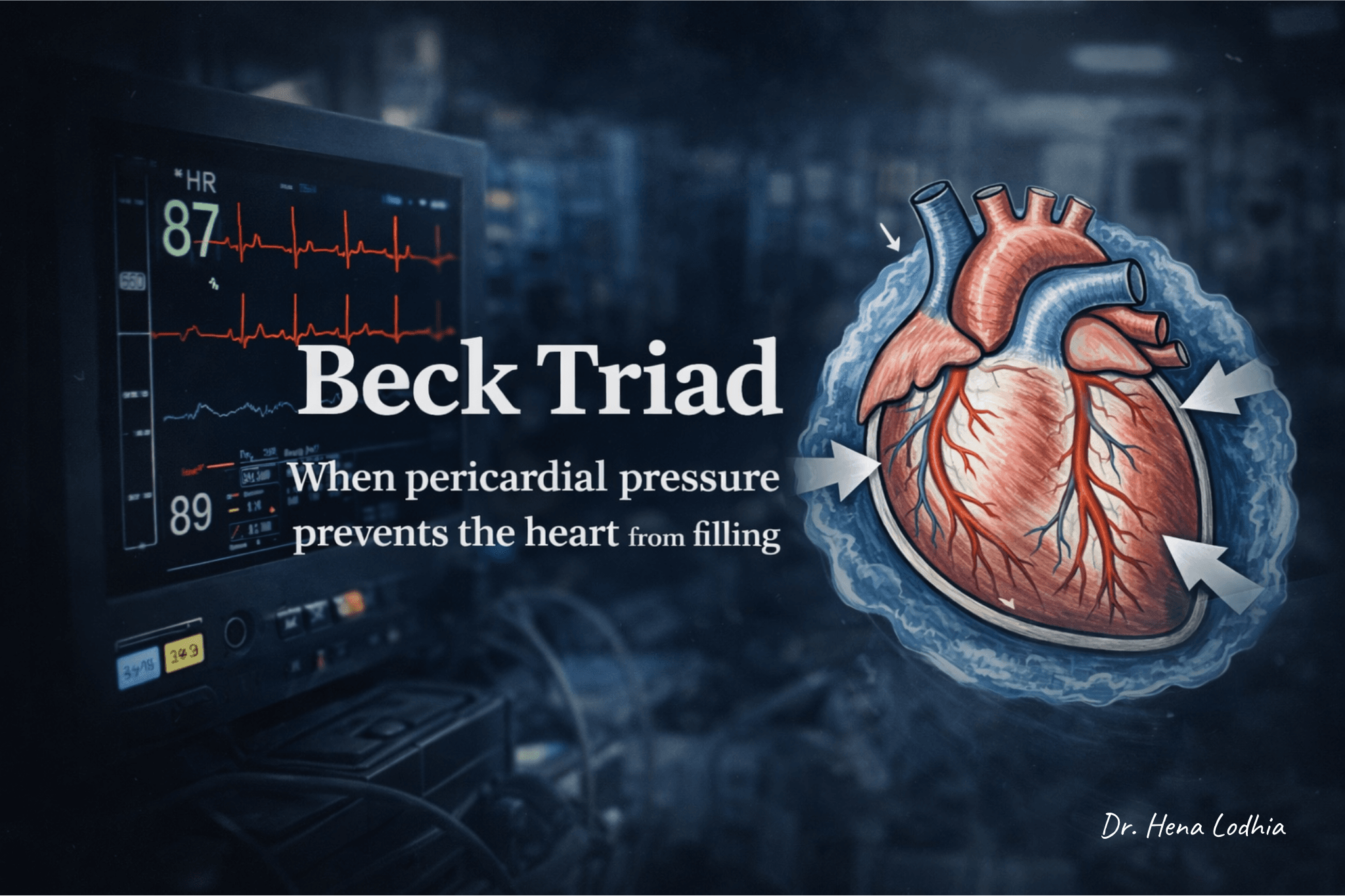
Beck Triad: When Low Blood Pressure and Full Neck Veins Tell the Same Story
A hypotensive patient often suggests hypovolemia. But when the neck veins are distended, something does not fit.
Low blood pressure with distended neck veins is unusual in hypovolemic shock and should raise concern for obstructive causes such as cardiac tamponade.
🎧 Clinical Summary Audio
Listen to the key concept in under 60 seconds.
The Atypical Presentation
A patient arrives hypotensive.
Naturally, you think of shock or volume loss. Low blood pressure usually means the body lacks adequate circulating blood.
But then you notice something unusual — the neck veins are distended.
That does not fit.
If blood pressure is low, veins should appear collapsed, not engorged.
This contradiction is the clue.
What is Beck Triad?
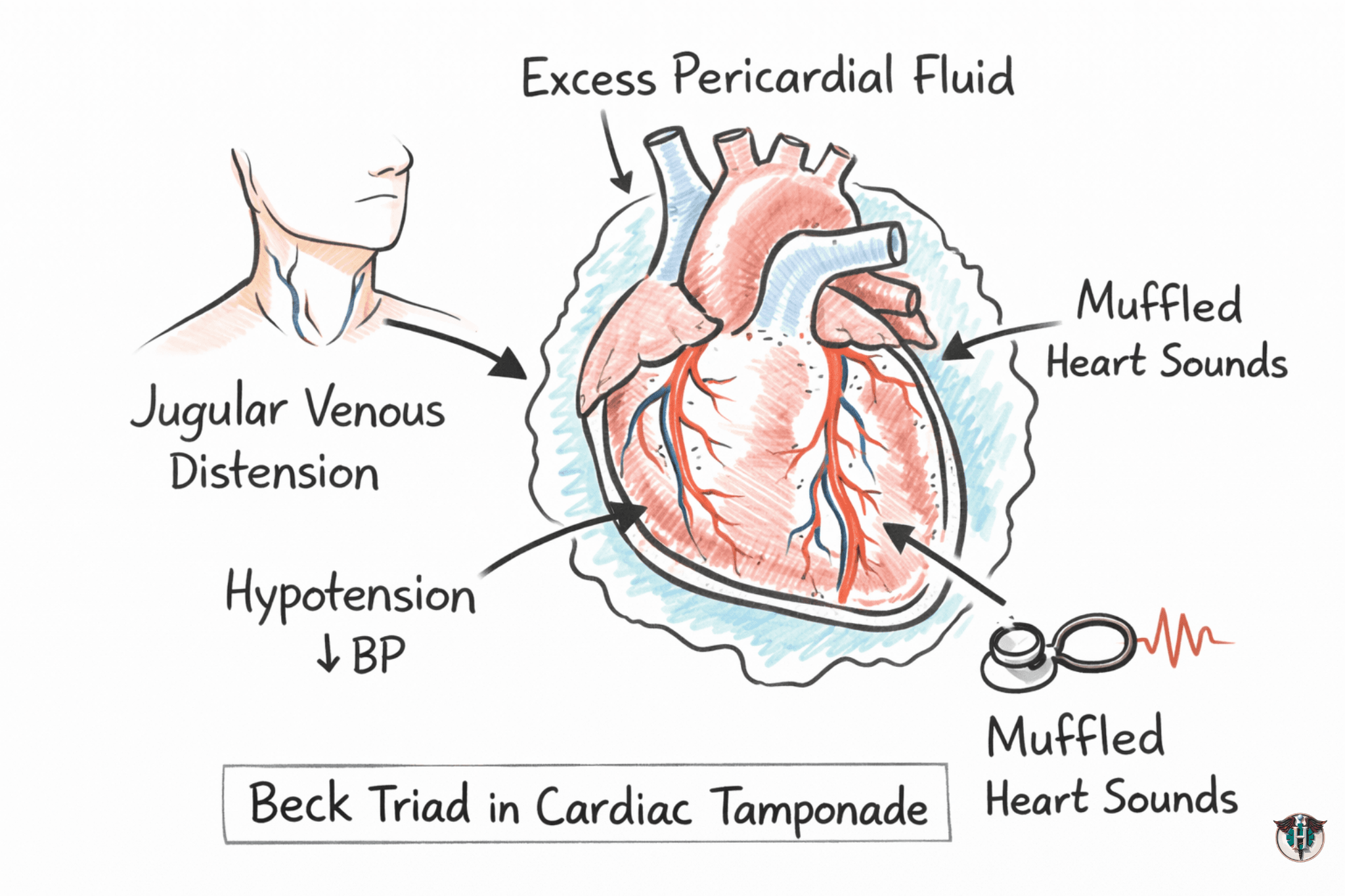
Beck triad is a classic clinical sign of cardiac tamponade, consisting of:
- Hypotension
- Jugular venous distension (JVD)
- Muffled heart sounds
Recognizing Beck triad can help raise suspicion for cardiac tamponade, although many patients do not present with all three findings.
The triad reflects impaired cardiac filling caused by rising pericardial pressure around the heart.
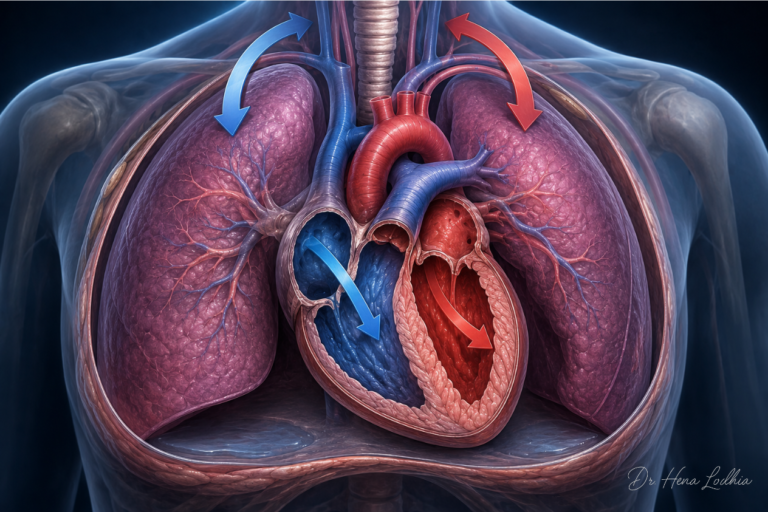
Understanding the Mechanism
Think of cardiac tamponade as a problem of external pressure on the heart.
Under normal circumstances, the ventricles relax during diastole and fill with blood. In cardiac tamponade, fluid accumulates within the pericardial sac and begins to compress the heart from the outside.
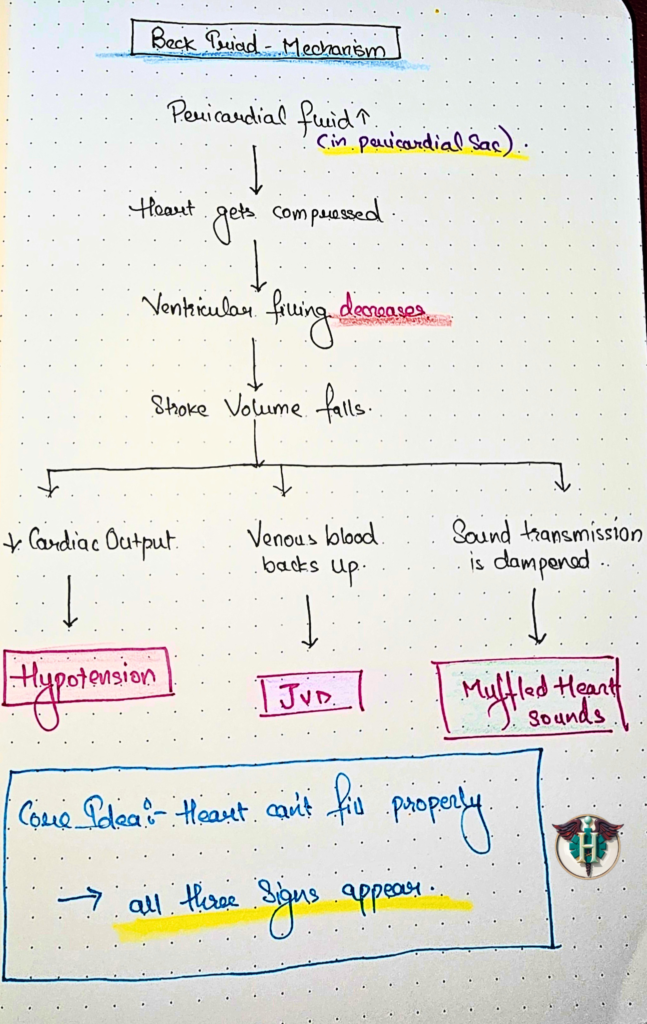
Flow of events
Fluid accumulates in the pericardial sac
→ The heart becomes compressed
→ The ventricles cannot fill properly during diastole
→ Stroke volume falls
From this single problem, all three components of Beck triad emerge.
1. Why hypotension occurs
When ventricular filling decreases, less blood is ejected with each heartbeat. This reduces stroke volume and cardiac output, eventually leading to hypotension.
Poor ventricular filling
→ Reduced stroke volume
→ Reduced cardiac output
→ Hypotension
2. Why jugular venous distension occurs
The compressed heart struggles to accept venous return. As blood backs up behind the heart, pressure rises within the venous circulation and becomes visible as distended neck veins.
Impaired cardiac filling
→ Venous blood backs up
→ Increased venous pressure
→ Jugular venous distension
3. Why heart sounds become muffled
The heart becomes surrounded by fluid within the pericardial sac. As sound travels through this fluid, its transmission is dampened, making heart sounds appear distant or muffled during auscultation.
Pericardial fluid accumulates
→ Sound transmission is dampened
→ Muffled heart sounds
Beck triad mechanism: Pericardial fluid compresses the heart, reduces ventricular filling, and leads to hypotension, jugular venous distension, and muffled heart sounds.
🩺 Compression of the heart = impaired filling
Everything in Beck’s triad comes from that single mechanism.
- ↓ Ventricular filling → Hypotension
- Venous backup → JVD
- Fluid around heart → Muffled sounds
Diagnosis of Cardiac Tamponade
Bedside echocardiography is the primary imaging modality for evaluating suspected cardiac tamponade and is the diagnostic test of choice.
Common echocardiographic findings include:
- Pericardial effusion
- Right atrial collapse (often an early sign)
- Right ventricular diastolic collapse
- A plethoric inferior vena cava (IVC) with reduced inspiratory collapse
Additional findings may include exaggerated respiratory variation in transvalvular flow velocities.
ECG may occasionally show electrical alternans, although this finding is neither sensitive nor specific for cardiac tamponade.
Quick Recall (Exam Focus)
Beck Triad is a classic finding in cardiac tamponade:
- Hypotension
- Jugular venous distension (JVD)
- Muffled heart sounds
Think: “The heart is compressed and cannot fill.”
Doctor’s Note
Hypotension with jugular venous distension (JVD) is not typical of hypovolemic shock. When these findings occur together, always consider obstructive causes, particularly cardiac tamponade.
Why This Matters Clinically
Beck’s triad represents the physiological consequences of a heart being compressed by pericardial fluid. Recognizing this pattern can help clinicians identify cardiac tamponade before severe hemodynamic deterioration occurs. While all three signs are not always present, their appearance should prompt urgent evaluation, as untreated tamponade can rapidly progress to obstructive shock and cardiovascular collapse.
Take It With You
Understanding a concept is one thing. Recalling it under exam pressure is another.
The Beck Triad Rapid Review PDF condenses everything on this page into a single high-yield revision sheet designed for quick review before exams, ward rounds, and viva preparation.
👉 Download the Beck Triad Rapid Review PDF
• Ready-to-write exam answer
• Visual mechanism flowchart
• One-page rapid revision sheet
Practice Point
Cardiac tamponade is a life-threatening emergency in which rising pericardial pressure impairs cardiac filling and reduces cardiac output.
Recognizing Beck’s triad at the bedside can help clinicians:
• Suspect cardiac tamponade early
• Prompt urgent diagnostic evaluation
• Prevent progression to obstructive shock and hemodynamic collapse
Frequently Asked Questions
CLINICAL REFERENCES
- 2015 ESC Guidelines for the Diagnosis and Management of Pericardial Diseases
- Adler Y, Charron P, Imazio M, et al. European Heart Journal. 2015;36(42):2921–2964. Acute Cardiac Tamponade (NEJM Review)
- Spodick DH. New England Journal of Medicine. 2003;349(7):684–690. Braunwald’s Heart Disease (Elsevier)
- Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, Braunwald E, eds. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Elsevier; 2021. Tintinalli’s Emergency Medicine (McGraw-Hill)
- Tintinalli JE, Ma OJ, Yealy DM, et al., eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 9th ed. McGraw-Hill Education; 2020. Cardiac Tamponade – StatPearls
- Sharma NK, Stashko E. StatPearls Publishing. Updated 2025.
References selected from peer-reviewed literature, major guidelines, and standard medical textbooks.

Educational Note
Medicine is more than memorising facts—it is understanding the physiological processes that connect symptoms, signs, investigations, and clinical outcomes.
This article is designed to help students, healthcare professionals, and curious learners develop deeper clinical reasoning by exploring the mechanisms behind disease. The goal is not only to improve examination performance but also to strengthen real-world diagnostic thinking and patient care.
Disclaimer
This content is provided for educational and informational purposes only. It is not intended to replace professional medical advice, diagnosis, or treatment.
Clinical decisions should always be based on individual patient evaluation, current evidence-based guidelines, institutional protocols, and professional judgment. While every effort has been made to ensure accuracy at the time of publication, medical knowledge continues to evolve, and readers should consult up-to-date references when making clinical decisions.
Go Deeper
Keeping up with medical research is difficult.
Thousands of new studies are published every year, yet most clinicians have limited time to read, analyze, and determine what truly matters for patient care.
Clinical Logic is a research-focused newsletter that breaks down important medical studies into clear, practical insights. Each edition translates complex research into plain language, highlighting what the findings mean, why they matter, and how they may influence clinical practice.
Whether you’re a student, resident, pharmacist, or practicing clinician, Clinical Logic helps you stay connected to the evolving world of medicine—without spending hours reading journals.