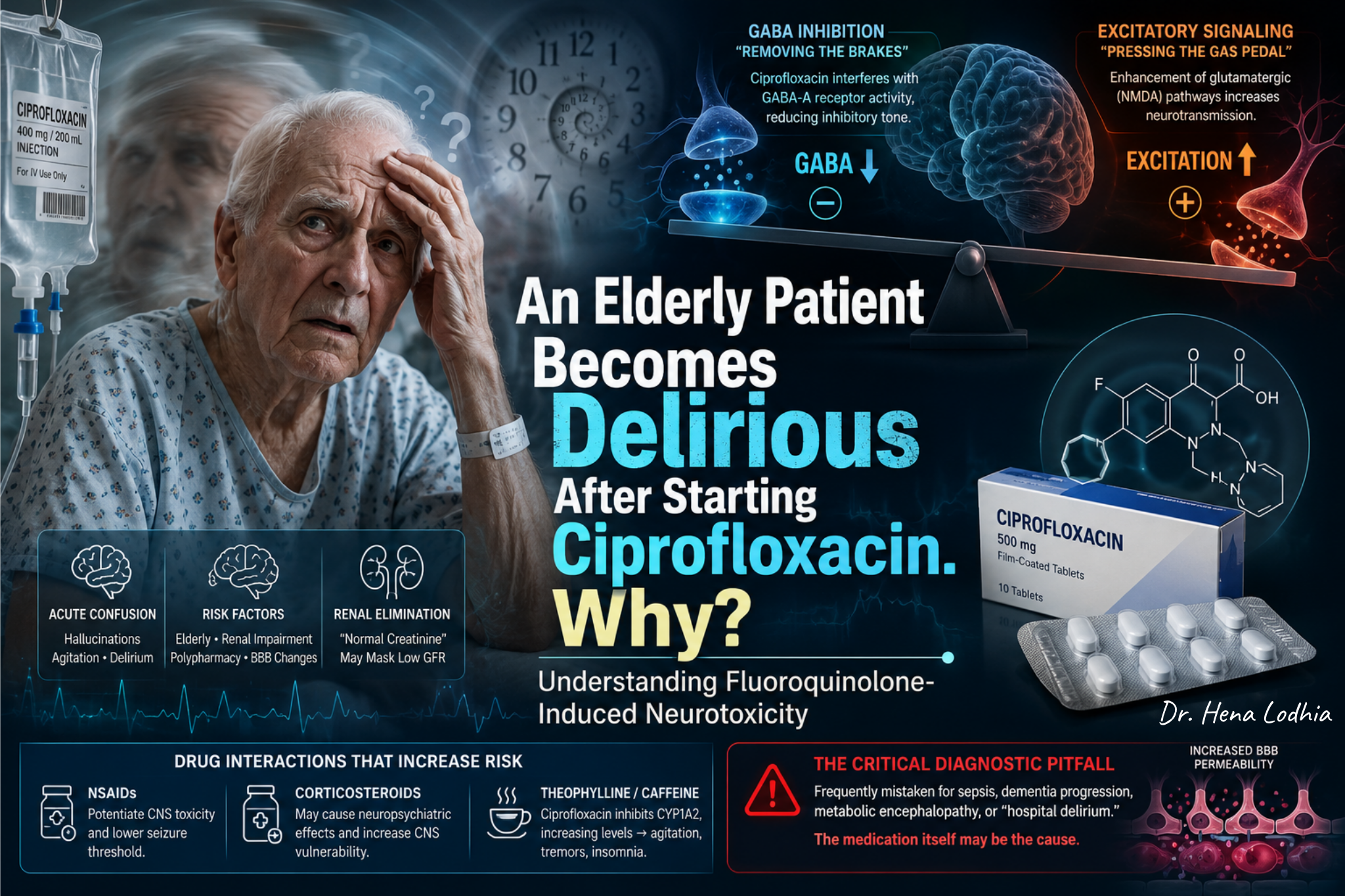
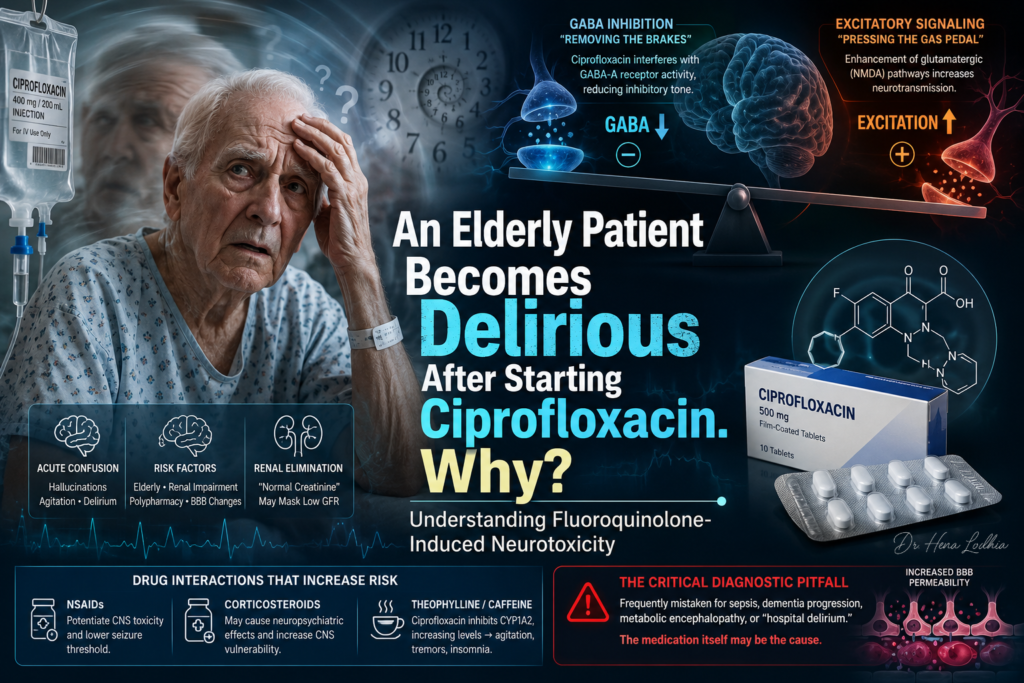
An elderly patient becomes delirious after starting ciprofloxacin. Why?
Fluoroquinolone-Induced Neurotoxicity: The Delirium Trap in Older Adults
🎧 Clinical Audio Summary: Ciprofloxacin Delirium in Older Adults
Listen to the key concept in under 60 seconds.
An 82-year-old patient is admitted with a urinary tract infection.
For the first two days, the clinical course appears reassuring. Fever improves. Blood pressure stabilizes. Inflammatory markers begin to fall. The antibiotic seems to be working.
Then, on the third day, the patient changes.
He becomes restless and suspicious. He speaks to people who are not in the room. He does not recognize his daughter. The nursing staff worry that the infection is worsening. The family fears that dementia has suddenly accelerated.
But the infection is not clearly deteriorating.
This is the diagnostic trap.
In an older hospitalized patient, delirium is often attributed to sepsis, dementia, dehydration, sleep deprivation, pain, urinary retention, constipation, hypoxia, metabolic disturbance, or the unfamiliar hospital environment. All of these possibilities must be assessed. But when acute neuropsychiatric symptoms appear shortly after a new medication is started, the medication chart becomes part of the neurological examination.
Ciprofloxacin is one of the drugs that should be checked.
Fluoroquinolones are effective antibiotics, but they are not neurologically neutral. They are associated with central nervous system and psychiatric adverse effects, including insomnia, agitation, confusion, hallucinations, paranoia, tremor, myoclonus, toxic psychosis, and seizures. These reactions may occur early, sometimes after initial exposure, and they are more likely to become clinically significant in patients with reduced neurological reserve.
The point is not that every confused elderly patient on ciprofloxacin has ciprofloxacin neurotoxicity. That would be unsafe reasoning. The point is that ciprofloxacin can be a reversible contributor to delirium when the timing fits, risk factors are present, and competing causes do not fully explain the clinical picture.
The Common Misconception
A common misconception is that antibiotics act only on bacteria.
That is not always true.
Antibiotics are designed to target microbial structures or enzymes. But some also interact with human physiology. Aminoglycosides can affect the inner ear and neuromuscular junction. Linezolid can interact with serotonergic pathways. Carbapenems and some cephalosporins can lower the seizure threshold, especially in renal impairment. Fluoroquinolones can affect the central nervous system.
Ciprofloxacin does not usually cause delirium by sedating the brain. The concern is closer to the opposite: a shift toward neuronal excitation.
The clinically useful sequence is:
Ciprofloxacin exposure
↓
Higher systemic or CNS exposure in a susceptible patient
↓
Interference with GABA-A-mediated inhibitory neurotransmission
↓
Relative dominance of excitatory signaling
↓
Lower threshold for network instability
↓
Insomnia, agitation, hallucinations, delirium, myoclonus, or seizures
This chain should not be read as a single mechanism that explains every case. Fluoroquinolone neurotoxicity is better understood as a convergence of drug exposure, renal clearance, CNS penetration, baseline brain vulnerability, systemic inflammation, and interacting medications.
The Mechanism: Loss of Inhibition, Excess Excitation
The brain depends on a controlled balance between inhibitory and excitatory signaling. This balance allows attention, perception, sleep-wake regulation, motor control, and behavior to remain organized.
GABA is the major inhibitory neurotransmitter in the adult brain. Through GABA-A receptor activity, neuronal firing is restrained. This inhibitory tone protects the brain from excessive cortical activation, agitation, perceptual disturbance, myoclonus, and seizures.
Fluoroquinolones are believed to interfere with GABA-A-mediated inhibitory neurotransmission. The safest phrasing is functional: ciprofloxacin can reduce GABAergic inhibitory restraint. That wording preserves accuracy without overstating one fixed receptor-level mechanism across all clinical contexts.
Once inhibitory restraint falls, neurons become easier to activate. A stimulus that would normally be tolerated may produce insomnia. Continued instability may produce anxiety, tremor, agitation, paranoia, or hallucinations. In severe toxicity, the same biological direction can progress toward myoclonus or seizures.
Excitatory pathways may also contribute. Experimental data suggest involvement of glutamatergic signaling, including NMDA-mediated pathways, but this should not be presented as a fully settled clinical mechanism. The important bedside point is that fluoroquinolone neurotoxicity moves the brain toward excitation, not sedation.
The mechanism can be framed as:
Reduced GABA-A-mediated inhibitory restraint
↓
Greater neuronal excitability
↓
Relative excess of excitatory signaling
↓
Cortical and subcortical network instability
↓
Disruption of attention, perception, sleep, behavior, and motor control
↓
Delirium, hallucinations, agitation, tremor, myoclonus, or seizures
This explains why the presentation often looks hyperactive. The patient may be sleepless, restless, suspicious, hallucinating, emotionally labile, or difficult to redirect. Hypoactive delirium can also occur, but it is more easily missed because the patient appears withdrawn, tired, or “quietly confused.”
Why the Elderly Are More Vulnerable
The elderly patient is not simply an older version of a younger adult. Aging changes pharmacokinetics, blood-brain barrier vulnerability, neurotransmitter reserve, and the clinical consequences of systemic stress.
The first issue is renal clearance.
Ciprofloxacin is significantly eliminated by the kidney, and impaired renal function increases drug exposure. In older adults, serum creatinine can be misleadingly normal because creatinine production depends on skeletal muscle mass. A frail, sarcopenic 82-year-old may generate little creatinine, so the laboratory value may appear reassuring even when true renal clearance is reduced.
This is the normal creatinine trap.
A serum creatinine of 0.7 mg/dL does not guarantee normal drug clearance in a frail older adult. Dosing should be guided by estimated renal function, and creatinine clearance using Cockcroft-Gault is often the more relevant calculation for drug dosing. The clinical context also matters: frailty, dehydration, acute kidney injury, low muscle mass, and fluctuating renal function can all change drug exposure.
The danger is not the creatinine number itself. The danger is assuming that a “normal” creatinine means normal pharmacokinetics. That assumption can allow silent drug accumulation.
The second issue is CNS reserve.
Older patients often have reduced resilience in multiple neurotransmitter systems. Baseline cognitive impairment, neurodegeneration, prior stroke, microvascular ischemic disease, sleep disruption, sensory impairment, and cholinergic vulnerability all reduce the brain’s ability to compensate for a new pharmacological insult. A drug effect that produces mild insomnia in a younger adult may precipitate florid delirium in an elderly patient with dementia or vascular brain disease.
The third issue is systemic inflammation.
During acute infection, inflammatory signaling can alter endothelial function, blood-brain barrier permeability, microglial activation, and cerebral neurotransmission. Ciprofloxacin is also handled by transport systems that help limit CNS exposure, including efflux mechanisms such as P-glycoprotein. Aging and systemic inflammation may weaken these protective barriers, so the same serum concentration may not produce the same CNS exposure in every patient.
This point should be interpreted clinically, not overextended. It does not mean every infected older patient develops high CSF ciprofloxacin levels. It means that acute illness can reduce the safety margin between therapeutic exposure and neurotoxicity.
The fourth issue is polypharmacy.
Older hospitalized patients are rarely exposed to one drug at a time. They may receive opioids, benzodiazepines, anticholinergics, dopamine-blocking antiemetics, corticosteroids, H2 blockers, antihistamines, gabapentinoids, or NSAIDs. Ciprofloxacin may not be the sole cause of delirium. It may be the final added burden that pushes a vulnerable brain past its compensatory limit.
The NSAID Interaction: A Critical Pharmacodynamic Amplifier
NSAIDs deserve specific attention because they are not merely “another medication” on the list.
Certain NSAIDs can potentiate fluoroquinolone-associated CNS toxicity through receptor-level interactions that further impair GABAergic inhibition. The interaction is pharmacodynamic: the combination can produce a greater reduction in inhibitory tone than either exposure alone.
Clinically, this matters because the combination is common. An elderly patient with a UTI may be prescribed ciprofloxacin while already taking ibuprofen, naproxen, or another NSAID for osteoarthritis, back pain, or fever. If agitation, tremor, myoclonus, hallucinations, or seizures appear soon afterward, the NSAID should not be dismissed as incidental.
The sequence is:
Ciprofloxacin exposure
↓
Reduced GABA-A-mediated inhibitory signaling
↓
Concomitant NSAID amplifies inhibitory failure
↓
Lowered delirium and seizure threshold
↓
Agitation, hallucinations, myoclonus, or seizures
This does not mean every patient receiving ciprofloxacin and an NSAID will develop neurotoxicity. It means the combination should raise clinical suspicion when the timing and phenotype fit.
Other Drug Interactions and Co-Exposures
Theophylline is a classic interaction. Ciprofloxacin can inhibit CYP1A2, reducing theophylline clearance. Elevated theophylline levels can produce tremor, insomnia, anxiety, nausea, tachycardia, seizures, and delirium. In a patient receiving theophylline, new agitation after ciprofloxacin should immediately raise concern for drug interaction and toxicity.
Caffeine is less dramatic but mechanistically relevant. Ciprofloxacin can reduce caffeine clearance through CYP1A2 inhibition. In susceptible patients, this may worsen insomnia, tremor, anxiety, or agitation. In an elderly hospitalized patient, sleep disruption alone can become a meaningful contributor to delirium.
Corticosteroids require a separate frame. They are independently associated with insomnia, mood change, agitation, psychosis, and delirium. When corticosteroids and fluoroquinolones are prescribed together, neuropsychiatric symptoms may be misattributed to infection alone. The combination is also classically associated with increased risk of tendinopathy and tendon rupture, which is a separate but important fluoroquinolone safety issue.
Anticholinergics reduce cognitive reserve by impairing cholinergic signaling, a key pathway for attention and arousal. Opioids may contribute through sedation, sleep fragmentation, hypercapnia, urinary retention, and constipation. Benzodiazepines can worsen delirium except in specific contexts such as alcohol or benzodiazepine withdrawal. Gabapentinoids can accumulate in renal impairment and produce somnolence, myoclonus, and confusion.
In practice, delirium is often not a single-drug story. The better question is not always, “Which drug caused this?” Sometimes the better question is, “Which new exposure tipped the balance?”
Clinical Pattern: What Should Make You Suspect Ciprofloxacin?
The most important clue is temporal association.
A patient starts ciprofloxacin. Within hours to days, new CNS or psychiatric symptoms appear. The earliest sign may not be obvious delirium. It may be insomnia, anxiety, restlessness, tremor, or emotional lability. Families may say, “This is not his usual behavior.”
Symptoms may include:
- New confusion or disorientation
- Inattention or fluctuating awareness
- Agitation, anxiety, paranoia, or emotional lability
- Visual or auditory hallucinations
- Insomnia or sleep-wake reversal
- Tremor or myoclonus
- Seizures
- Sudden cognitive worsening after antibiotic initiation
The phenotype may be hyperactive, hypoactive, or mixed. Hyperactive delirium is recognized earlier because it disrupts the ward. Hypoactive delirium is more easily missed because the patient appears tired, withdrawn, depressed, or “just old.”
There is no single laboratory test that confirms ciprofloxacin delirium. The diagnosis is clinical and probabilistic. It depends on timing, risk factors, renal function, medication review, exclusion of competing causes, and improvement after dose adjustment or withdrawal of the suspected agent.
The Diagnostic Pitfall: Anchoring on Infection
The major pitfall is anchoring.
An elderly patient with infection becomes confused. The team assumes the infection is worsening. Antibiotics are escalated. More drugs are added. Sleep deteriorates. The patient becomes more delirious. The original medication trigger is never reconsidered.
This is dangerous because infection-related delirium and drug-induced delirium require different actions.
If the infection is worsening, the patient may need source control, repeat cultures, imaging, broader antimicrobial coverage, hemodynamic reassessment, oxygenation support, or ICU-level care.
If the antibiotic is contributing to delirium, the patient may need dose adjustment, discontinuation, renal reassessment, removal of interacting drugs, or substitution with a safer appropriate antimicrobial.
Both can be true at the same time. Ciprofloxacin toxicity does not exclude sepsis. Sepsis does not exclude ciprofloxacin toxicity.
The safest approach is parallel thinking:
Is the infection improving or worsening?
Are vital signs stabilizing or deteriorating?
Are inflammatory markers falling or rising?
Is there hypoxia, hypoglycemia, hyponatremia, hypercalcemia, uremia, hepatic dysfunction, or acidosis?
Is there pain, urinary retention, constipation, or sleep deprivation?
Has stroke, intracranial bleeding, seizure, or nonconvulsive status epilepticus been considered when appropriate?
Which medications were started, stopped, or dose-adjusted before the mental status changed?
Is ciprofloxacin still necessary?
Is the dose appropriate for renal function?
Are NSAIDs, theophylline, steroids, anticholinergics, sedatives, or other CNS-active drugs present?
This is how clinicians avoid missing reversible iatrogenic delirium.
Clinical Approach
When an elderly patient develops new delirium after starting ciprofloxacin, the first step is urgent reassessment, not automatic attribution.
Check vital signs, oxygenation, hydration, glucose, electrolytes, renal function, hepatic function, inflammatory trend, urine output, pain, urinary retention, constipation, and sleep disruption. Review the full medication chart, including PRN medications. Delirium often hides in the “as needed” section.
Assess whether ciprofloxacin is still indicated. Was it started empirically? Are culture results available? Is the infection uncomplicated cystitis, pyelonephritis, prostatitis, catheter-associated UTI, bacteremia, or resistant gram-negative disease? Is there a narrower option based on susceptibility data and local antimicrobial guidance?
Review renal dosing carefully. Do not rely only on serum creatinine. Estimate renal function, consider Cockcroft-Gault creatinine clearance for drug dosing when appropriate, and reassess the dose in the context of frailty, sarcopenia, dehydration, and acute illness.
If ciprofloxacin neurotoxicity is suspected, clinicians should consider stopping ciprofloxacin or changing to an appropriate non-fluoroquinolone alternative when clinically feasible. The replacement should be guided by infection site, culture susceptibility, renal function, allergy history, local resistance patterns, and illness severity.
For example, an inpatient with susceptible Enterobacterales pyelonephritis may be suitable for ceftriaxone. A sicker patient with broader gram-negative risk may require a different empiric agent such as piperacillin-tazobactam, depending on local resistance patterns and pseudomonal risk. A stable patient with uncomplicated lower UTI may be eligible for oral options such as nitrofurantoin when renal function is adequate, or fosfomycin when appropriate. These are examples, not automatic substitutions.
Remove amplifiers. Stop unnecessary NSAIDs. Check for theophylline exposure. Reduce anticholinergic burden. Reassess opioids, sedatives, antiemetics, antihistamines, gabapentinoids, and corticosteroids. Correct dehydration, hypoxia, metabolic disturbances, constipation, urinary retention, and sleep disruption.
Supportive delirium care is not cosmetic. Reorientation, mobilization, hearing aids, glasses, sleep protection, hydration, pain control, family presence, and avoidance of unnecessary restraints reduce the background burden on an unstable brain.
Symptoms often improve after withdrawal of the offending agent and drug clearance, but recovery is not always immediate. Persistent symptoms may occur in severe toxicity, renal impairment, advanced age, CNS disease, or multifactorial delirium.
Historical and Safety Context
Fluoroquinolones became widely used because they were convenient and powerful: broad spectrum, high oral bioavailability, good tissue penetration, and useful gram-negative coverage. Ciprofloxacin in particular became associated with the idea of a “strong UTI antibiotic.”
That historical convenience created overuse.
Over time, the adverse effect profile became harder to ignore. Fluoroquinolones are now associated not only with tendinopathy and tendon rupture, but also with peripheral neuropathy, neuropsychiatric reactions, dysglycemia, and other potentially serious adverse effects.
Regulatory agencies have progressively strengthened warnings and restrictions around systemic fluoroquinolone use. The FDA has warned that systemic fluoroquinolones should be reserved for certain uncomplicated infections when no alternative treatment options are available because serious adverse effects may outweigh benefits in those settings. The EMA also reviewed serious, disabling, and potentially permanent adverse effects and recommended restrictions on quinolone and fluoroquinolone use.
The modern lesson is not that fluoroquinolones should never be used. They remain valuable drugs when the indication is appropriate. The lesson is that they should not be used casually when safer effective alternatives exist, especially in older adults with frailty, renal vulnerability, CNS disease, or polypharmacy.
Antimicrobial stewardship is therefore part of neuroprotection.
Avoiding unnecessary fluoroquinolone exposure is not only about preventing resistance. It is also about preventing avoidable adverse drug events in patients whose brains, kidneys, tendons, nerves, and glucose regulation may be less resilient than they appear.
The Clinical Lesson
When an elderly patient becomes delirious after starting ciprofloxacin, do not jump to one explanation.
Do not assume it is dementia.
Do not assume it is sepsis.
Do not assume it is hospital confusion.
Do not assume the antibiotic is innocent because it is treating the infection.
Think mechanistically.
Ciprofloxacin can enter the CNS. In susceptible patients, it may impair GABA-A-mediated inhibitory signaling and shift the brain toward excitation. NSAIDs and other interacting drugs can amplify this effect. Renal impairment can increase exposure, especially when sarcopenia makes serum creatinine look deceptively normal. Aging, vascular brain disease, dementia, systemic inflammation, sleep disruption, and polypharmacy reduce neurological reserve.
The result may be acute delirium, hallucinations, agitation, tremor, myoclonus, or seizures.
The key clinical move is to recognize the timing.
A new mental status change after a new medication is not automatically disease progression. Sometimes the treatment has become part of the pathology.
Frequently Asked Questions (FAQ)
Educational Note
CLINICAL REFERENCES
- Wierzbiński P, Więckowska B, Kortas-Stempak B, Hacia M, Śliwińska-Mossoń M.Depressive and Other Adverse CNS Effects of Fluoroquinolones.Pharmaceuticals (Basel). 2023;16(8):1105.DOI: 10.3390/ph16081105
- Anwar AI, Alwafi H, Samannodi M, et al.Fluoroquinolones: Neurological Complications and Side Effects in Clinical Practice.Cureus. 2024;16(3):e56309.DOI: 10.7759/cureus.56309
- Baggio D, Ananda-Rajah MR.Fluoroquinolone Antibiotics and Adverse Events.Australian Prescriber. 2021;44(5):161–164.DOI: 10.18773/austprescr.2021.039
- U.S. Food and Drug Administration (FDA).FDA Approves Safety Labeling Changes for Fluoroquinolones.FDA Drug Safety Communication. 2016.FDA Safety Information Link
- European Medicines Agency (EMA).Fluoroquinolone Antibiotics: Reminder of Measures to Reduce the Risk of Long-Lasting, Disabling and Potentially Irreversible Side Effects.European Medicines Agency. 2023.EMA Press Release Link
- Wanleenuwat P, Suntharampillai N, Iwanowski P.Antibiotic-Induced Epileptic Seizures: Mechanisms of Action and Clinical Considerations.Seizure. 2020;81:167–174.DOI: 10.1016/j.seizure.2020.08.010
- Jay GT, Azimaee M.Ciprofloxacin-Induced Delirium.Annals of Pharmacotherapy. 2023;57(5):610–614. (First published online 2022)DOI: 10.1177/10600280221115317
📖 Further Reading
- Rusu A, Munteanu AC, Uivarosan D, et al.Overview of Side-Effects of Antibacterial Fluoroquinolones.Antibiotics (Basel). 2023;12(5):916.DOI: 10.3390/antibiotics12050916
- Rissardo JP, Caprara ALF.Fluoroquinolone-Associated Movement Disorder: A Literature Review.Toxics. 2023;11(5):455.DOI: 10.3390/toxics11050455
- Xie WL, et al.Psychiatric Disorders Associated with Fluoroquinolones: A Pharmacovigilance Analysis Based on FAERS.Frontiers in Pharmacology. 2022;13:1044345.DOI: 10.3389/fphar.2022.1044345
- Schmuck G, Schürmann A, Schlüter G.Determination of the Excitatory Potencies of Fluoroquinolones in the Central Nervous System: An In Vitro Approach.Antimicrobial Agents and Chemotherapy. 1998;42(7):1831–1836.DOI: 10.1128/AAC.42.7.1831
- Davey PG, Charter M, Kelly S, et al.Ciprofloxacin and Sparfloxacin Penetration into Human Brain Tissue and Their Activity as Antagonists of GABA-A Receptors.Antimicrobial Agents and Chemotherapy. 1994;38(11):2615–2622.DOI: 10.1128/AAC.38.11.2615
References selected from peer-reviewed literature, major guidelines, and standard medical textbooks.

Medicine is more than memorizing facts—it is understanding the physiological and pathological processes that connect symptoms, signs, investigations, treatments, and clinical outcomes.
This article is intended to help students, healthcare professionals, and curious learners develop deeper clinical reasoning by exploring the mechanisms underlying disease. The goal is not only to improve examination performance, but also to strengthen diagnostic thinking, therapeutic decision-making, and patient care.
Disclaimer
This content is provided for educational and informational purposes only. It is not intended to replace professional medical advice, diagnosis, or treatment.
Clinical decisions should always be based on individual patient assessment, current evidence-based guidelines, institutional protocols, and professional judgment. While every effort has been made to ensure accuracy at the time of publication, medical knowledge continues to evolve, and readers are encouraged to consult up-to-date references and relevant clinical resources when making healthcare decisions.
The views and explanations presented in this article are intended to facilitate learning and clinical understanding. They should not be interpreted as specific medical recommendations for any individual patient.
Go Deeper
Keeping up with medical research is difficult.
Thousands of new studies are published every year, yet most clinicians have limited time to read, analyze, and determine what truly matters for patient care.
Clinical Logic is a research-focused newsletter that breaks down important medical studies into clear, practical insights. Each edition translates complex research into plain language, highlighting what the findings mean, why they matter, and how they may influence clinical practice.
Whether you’re a student, resident, pharmacist, or practicing clinician, Clinical Logic helps you stay connected to the evolving world of medicine—without spending hours reading journals.
Join Clinical Logic and let the research come to you.